Managing rheumatoid arthritis
Rheumatoid arthritis is not curable. However, early treatment is effective in managing symptoms and slowing down disease progression. Read on to find out more.
Keep track of medicines and access important health info any time and anywhere, especially in emergencies.
Rheumatoid arthritis is not curable. However, early treatment is effective in managing symptoms and slowing down disease progression. Read on to find out more.
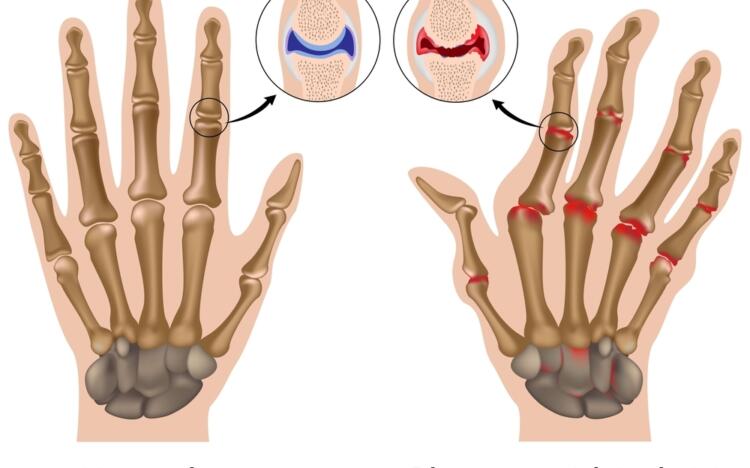
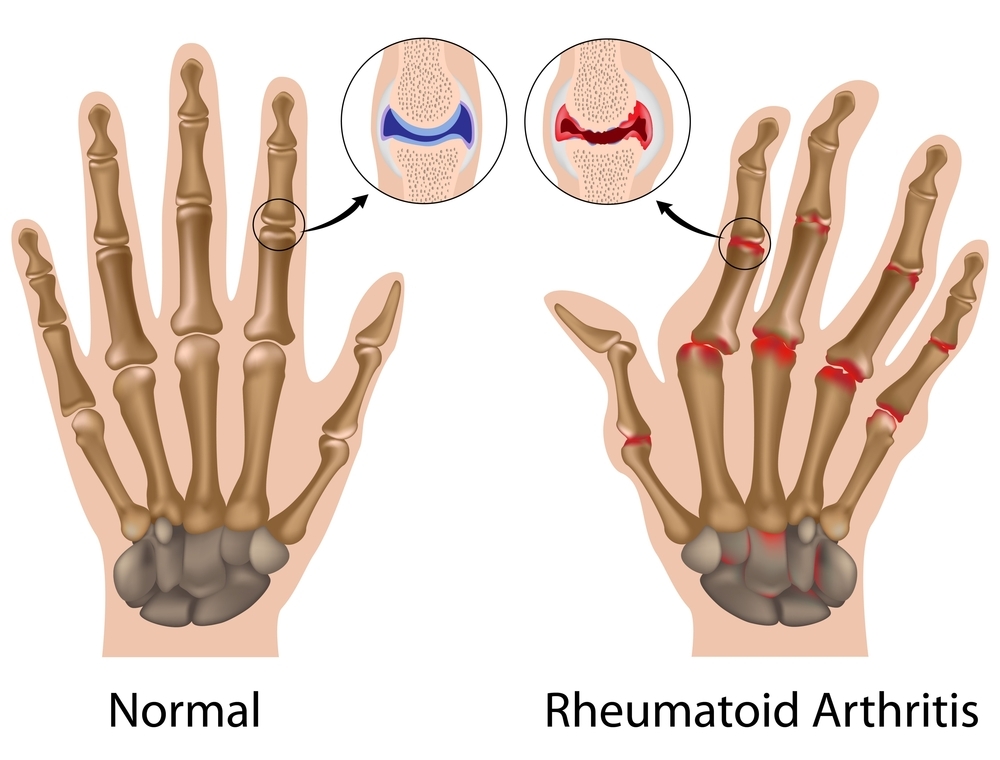
Rheumatoid arthritis (RA) is a long-term (chronic) autoimmune condition. This means the body’s immune system, which usually fights infection, attacks the lining of the joints, causing them to become inflamed and damaged.
Around 2% of the population are estimated to have RA. The disease usually develops between the ages of 35 and 60 years. In Australia, most people who have the condition are over the age of 65.
RA most commonly affects smaller joints in the hands, wrists and feet although larger joints such as the hips and knees can also be affected. Some people also experience problems in other parts of the body including the skin, eyes, lungs, heart and kidneys.
Symptoms of RA can vary from person to person. Common symptoms include:
It’s not known exactly what causes rheumatoid arthritis (RA).
People are thought to be at an increased risk of developing the condition if they:
It can be difficult to diagnose rheumatoid arthritis (RA). The symptoms are similar to many other conditions.
It’s important that a definite diagnosis is made early so that treatment can be started quickly.
A diagnosis of RA is primarily based on your symptoms and a physical examination of your joints by your doctor. Your doctor will use blood tests to help confirm the clinical diagnosis.
Blood tests can detect signs of inflammation in the joints as well as certain proteins – antibodies – which are made by the body’s immune system.
X-rays are often taken as they can show the extent of joint damage. However, in the early stages of disease, X-rays may not show any joint damage.
If a GP suspects someone has RA, they will usually refer them to a rheumatologist. Rheumatologists are doctors who specialise in arthritis.
There is currently no cure for rheumatoid arthritis (RA) but treatment can help reduce joint inflammation and decrease pain and stiffness.
Starting medicines in the early stages of disease prevents permanent joint damage and improves the quality of life of people living with RA.
The type of medicines used will depend on a number of factors that determine how active the disease is and how likely it is to cause joint damage. Rheumatologists will often test different types of treatment to see which one works best. There are several types of medicine used to treat RA.
Disease-modifying antirheumatic drugs (DMARDs) are a group of medicines that are usually given to people when first diagnosed with RA (see Table 1). These medicines reduce the activity of the immune system which is attacking and damaging healthy joints.
Methotrexate is a type of DMARD and is the recommended medicine for most people. It’s usually taken in the form of a tablet but can also be injected (just under the skin, not into a muscle or the blood stream). Methotrexate can be used in combination with other medicines, such as biological DMARDS (bDMARDS).
| DMARD | Use |
|---|---|
| Conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) eg, methotrexate | The first-line medicine for reducing joint damage and improving symptoms in early RA. Often given alongside other DMARDs. |
| Biological disease-modifying antirheumatic drugs (bDMARDS) eg, adalimumab, etanercept | Second-line medicine in RA. They are given as injections and are only used if other DMARDs are not working properly. |
| Targeted synthetic disease-modifying antirheumatic drugs (tsDMARDS) eg, tofacitinib | Also a second-line medicine in RA. They are given orally and may be used in place of csDMARDs and bDMARDs. |
Steroids, such as prednisone, can reduce inflammation in the joints and provide quick relief of symptoms. However, they’re only used short term to provide pain relief while waiting for DMARD medication to work. This is because long-term use of steroids is linked with serious side effects.
Non-steroidal anti-inflammatory drugs (NSAIDs) are also given to people with RA to relieve pain and reduce inflammation in the joints. NSAIDs are only prescribed to help symptoms and do not slow down disease progression. Check with your doctor or pharmacist before taking NSAIDs over the counter particularly if you have problems with your blood pressure, heart, kidneys or stomach.
There are many myths about methotrexate which can cause great concern and can be a barrier to treatment.
Table 2 below includes facts which bust some of the most common myths about methotrexate for the treatment of rheumatoid arthritis (RA).
| Fact | Myth |
|---|---|
| Methotrexate takes time to work – a response to therapy can take 6–12 weeks. | Methotrexate works straightaway. |
| Methotrexate in RA is used in low doses – it’s not considered chemotherapy. | Methotrexate is chemotherapy. |
| Methotrexate (in low doses) has been used safely and effectively for RA since its introduction in the 1950s. | Methotrexate is toxic. |
| People receiving low dose methotrexate for RA can safely make contact with pregnant women. | People receiving methotrexate should not make contact with pregnant women. |
| Methotrexate can be safely taken with non-steroidal anti-inflammatory drugs (NSAIDs). | Methotrexate should not be taken alongside NSAIDs. |
| If required, methotrexate injections can be safely self-administered. | Self-administration of methotrexate injections is unsafe |
Like all medicines, methotrexate may cause side effects. The most common side effects include:
Side effects from methotrexate can be reduced by taking it with food or in the evening. If you are concerned about side effects of your medicine, speak to your doctor or rheumatologist.
Information that comes with your medicine may mention serious side effects that can occur with methotrexate. However, many of these side effects relate to high-dose methotrexate, which is often used for the treatment of cancer. Methotrexate is used in much lower doses for the treatment of RA and serious side effects may not apply.
Dosing errors can and have occurred with oral methotrexate. Always confirm the dose and how often to take it with your doctor and/or your pharmacist before starting your medicine.
More information about dosages of methotrexate is available on the TGA website
People with rheumatoid arthritis (RA) should make regular appointments with their rheumatologist. Routine tests are often required to check that treatment is working properly and to minimise any side effects of treatment.
You should also speak to your GP or rheumatologist if you plan on taking any other medicines at that same time as those your doctors have prescribed to treat your RA. Other medicines include over-the-counter, herbal and naturopathic medicines. Check that these will not interfere or interact with your RA medicine.
In some cases, urgent medical attention may be required. You should contact your doctor or rheumatologist if you experience any of the following:
You can take action to help prevent and reduce the impact of rheumatoid arthritis (RA) on your quality of life.