Article
Administration of medicines to children: a practical guide
- Lucinda Smith, Catherine Leggett, Corey Borg
- Aust Prescr 2022;45:188-92
- 30 November 2022
- DOI: 10.18773/austprescr.2022.067
Getting children to take medicines can be difficult. There is no ‘one-size-fits-all’ approach.
When selecting medicines for children, it is important to consider the child’s age, swallowing ability, ease of administration and accessibility of the product.
Ask the child, parent or caregiver about their preference for formulations and flavours.
There are different ways to alter the taste, aftertaste and mouth feel of medicines, which may help improve palatability.
Pharmacists or medicines information services can assist with advice on suitable formulations or methods of administration.
Giving medicines to infants and children can be challenging. Children may refuse to take medicines for many reasons, such as fear, taste, embarrassment or inconvenience.
This problem is compounded by a lack of suitable formulations for paediatrics, restricting prescribing options and posing safety concerns. There is also limited information for parents and caregivers on how to give medicines to children, with most information coming from experience and anecdotal reports.
There is a well-recognised lack of suitable paediatric formulations available,1 contributing to an increased risk of dosing errors and difficulties in administration. When selecting medicines for children, it is important to consider factors such as the child’s age, swallowing ability, ease of administration and accessibility of suitable formulations of the product. Understanding the characteristics of each formulation can assist with choosing the most appropriate medicine for a child.
Oral liquids are the preferred formulation for younger children as they are easier to swallow2 and allow for flexible dosing based on the child’s age and weight. Liquids may also be mixed with different flavours at the time of administration to help mask the taste and smell of a medicine.
However, liquid formulations are not without risk and can result in over- or underdosing, particularly in the following cases:
Oral liquids may contain excipients such as colourings, solvents and preservatives at concentrations that may not be suitable for children.5 For example, furosemide (frusemide) oral solution contains 12.7% ethanol, which is typically considered insignificant in adults. However, it exceeds the maximum allowed ethanol content of 0.5% for children younger than six years of age, limiting the use of the proprietary furosemide (frusemide) product in this age group.6
Oral liquids often contain sugars to help improve palatability. It is important to consider the effects of sugar on teeth, particularly with chronic medicines. To minimise dental cavities, consider sugar-free formulations and encourage children to brush their teeth after taking a dose.7
If an oral liquid is not available, alternative oral formulations may be suitable. If a solid dosage form requires manipulation (chewing, crushing, dispersing, halving or breaking) to facilitate administration, particular drug properties should be considered:
Tablets are a suitable alternative to oral liquids,
particularly when medicines are unpalatable.8 However, a child’s
ability to swallow tablets must be considered. There
is no established age at which children are able to
swallow tablets, as it is a skill that must be
learned.9 Several
resources are available for caregivers to assist
with teaching children to swallow tablets or
capsules (see Box). Some children
may be able to swallow tablets from a young age,
although most children are usually at least 8–10
years of age before they can routinely take
tablets.10 If
prescribing or dispensing for a child, the child or
carer should always be asked if they would prefer
tablets or oral liquids.
Tablets are more accessible with easier storage and transport options than those for oral liquids. However, tablets have limited dose flexibility, decreasing the ability to prescribe weight-based doses.5
Most tablets are intended to be swallowed whole, but some immediate-release preparations may be chewed, crushed, or halved or quartered using a tablet cutter.5 Caution should be taken when manipulating tablets as this may result in a small portion of the dose being lost. This is particularly significant when giving medicines with a narrow therapeutic index. Additionally, most tablets are not formulated to be palatable, so crushing or dispersing them may impact a child’s willingness to take the medicine.
Modified-release tablets should be swallowed whole, as chewing or crushing them may damage the modified-release formulation, causing toxicity by releasing the total amount of medicine at once.11
Some children may find capsules easier to swallow than tablets. However, capsules cannot be halved, which limits their dose flexibility.
Most capsules are formulated to be swallowed whole. Some hard capsules (filled with powder or coated granules) may be opened and their contents mixed or sprinkled in food or drinks. Similarly, some soft capsules (filled with liquids or semisolids) may be chewed (e.g. colecalciferol).5
Oro-dispersible dosage forms, including tablets, wafers and films, are formulated to disperse rapidly once placed on the tongue. Alternatively, they can be dispersed in a small volume of liquid before administration. These preparations may be useful in children, as they do not need to be swallowed whole or crushed.5
Oro-dispersible medicines are commonly formulated with additive flavours to help mask the taste. Due to their delicate composition, it may be difficult to half or quarter these dosage forms, limiting their dose flexibility.
Table 1 - Common recommendations and precautions for administering medicines to children
|
Recommendations |
Precautions |
|
Oral liquids, suspensions and elixirs |
|
|
Use metric measures, such as a medicine syringe or cup |
Do NOT use everyday utensils, such as teaspoons or tablespoons |
|
Count oral drops on a spoon before administering |
Do NOT administer drops directly from the bottle into the child’s mouth |
|
Mix oral liquids with a small amount of water or juice |
Do NOT mix the medicine in large volumes |
|
If the medicine is available in multiple flavours, ask the child for their preference |
Do NOT mix the medicine with a child’s essential foods (e.g. milk or formula), as the altered taste may cause future aversion to the essential foods |
|
Tablets, capsules and solid dosage formulations |
|
|
Place the tablet in the middle of the tongue and follow with a large volume |
Do NOT mix with honey in children younger than one year of age due to the potential risk of infant botulism |
|
Try drinking a small amount of liquid from a bottle or using a straw |
Do NOT give large volumes (i.e. aim for one mouthful) |
|
Try halving or quartering tablets |
Do NOT break modified-release, cytotoxic or hazardous medicines |
|
Crush tablets between two spoons and mix with a small amount of soft food |
Do NOT crush modified-release, cytotoxic or hazardous medicines |
|
Try dispersing the tablet in a small volume of liquid (water or juice) |
|
|
Check with a pharmacist if the tablets can be crushed or the capsules opened |
|
|
Encourage parents and caregivers to teach children how to swallow tablets. There are several resources to assist with teaching children to swallow solid dosage forms (see Box) |
|
Taste is a powerful deterrent for children and is
thought to have evolved as a safeguard against
ingesting toxic substances.13 The unpleasant
taste of a medicine can be improved by mixing it
with various flavoured syrups or cordials (Table 2).6,7
However, the child’s taste preferences must be
considered before mixing with flavours. Liquorice,
peppermint and coconut flavours may taste reasonable
to adults but may be disliked by children.14
Table 2 - Tastes and masking flavours
|
Taste of the medicine |
Examples* |
Flavour to mask the taste of the medicine |
|
Sour |
Multivitamins (e.g. vitamin C) |
Cherry, lemon, lime, mandarin, orange, strawberry, raspberry, pineapple |
|
Bitter |
Antibiotics |
Cherry, chocolate, liquorice, strawberry, peach, coffee, mint, lemon, lime, raspberry, tutti-frutti, orange, cinnamon |
|
Sweet |
Lactulose |
Caramel, lemon, orange, vanilla, bubble-gum |
|
Salty |
Iron supplements
Antihistamines |
Banana, caramel, cream, chocolate, grape, vanilla, raspberry, orange, cinnamon, nut, butter, butterscotch, maple |
|
Any |
Spreadable yeast extract, peanut butter, jam, honey, apple sauce, custard, ice cream |
|
* Common examples are based on patient reports, although any drug may be considered ‘bad’ tasting depending on subjective taste preferences.
Mixing medicines with a small amount of food or liquid is unlikely to cause drug–food interactions, even with medicines recommended to be given on an empty stomach (e.g. flucloxacillin). A small reduction in absorption of the medicine will pose less of a problem than that created by a child refusing to take the medicine at all.
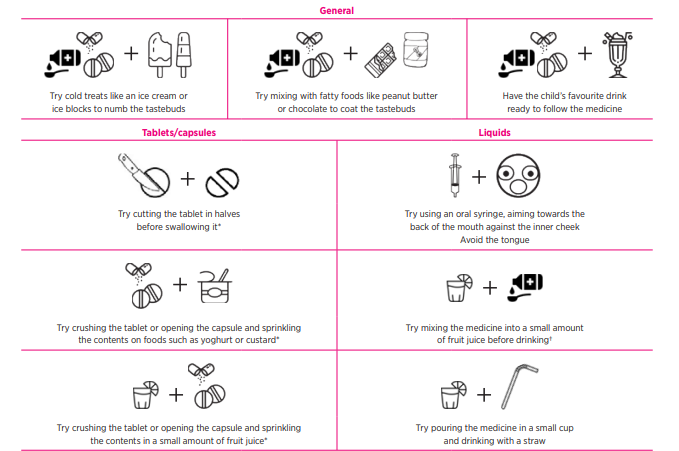
The aftertaste of a medicine is a difficult issue to navigate, particularly if it prevents a child from accepting subsequent doses.13,14 When administering a medicine, try and avoid the tongue, aiming oral liquids towards the back of the mouth against the cheek. Alternatively, consider swapping to a capsule or tablet formulation, which can be swallowed whole. Some children may find it more palatable to take a medicine via a straw or follow with a cold drink to lessen the aftertaste.
The mouth feel of a medicine may also be a deterrent for some children. To improve the feel of oral liquids, consider diluting in water or a flavoured drink to reduce their viscosity.13,14 To combat the grittiness of crushed tablets or granules, try mixing with thick or gelatinous foods such as jelly, custard or spreads.
When prescribing medicines for children, some practical considerations include:
There are several techniques and strategies that can be used to improve the palatability and acceptance of medicines by children. Often, there is no single solution, and instead, there are many strategies that may be implemented by the parent or caregiver. Further guidance may be obtained from the local pharmacist or medicines information service.
Acknowledgements: Sean Turner (Director of Pharmacy), David Ellis (Senior specialist pharmacist (Manufacturing and Psychiatry)) and Lynn Costi (Senior pharmacist, Medicines Information Service), SA Pharmacy, Women’s and Children’s Hospital Campus, SA Health.
Conflicts
of interest:
none
declared
This
article is peer-reviewed.
Australian Prescriber welcomes Feedback.

Senior pharmacist, Medicines Information Service, SA Pharmacy, Women’s and Children’s Hospital Campus, SA Health, Adelaide
Medicines information manager, Medicines Information Service, SA Pharmacy, Women’s and Children’s Hospital Campus, SA Health, Adelaide
Senior pharmacist, Medicines Information Service, SA Pharmacy, Women’s and Children’s Hospital Campus, SA Health, Adelaide