Editorial
Antimicrobial use and resistance in Australia
- John Turnidge
- Aust Prescr 2017;40:2-3
- 1 February 2017
- DOI: 10.18773/austprescr.2017.007
Managing the emergence
and increasing resistance to antimicrobials in hospitals and the community has
become an urgent national and international problem.1 As part of a plan to
tackle this, Australia is developing a coordinated national program to monitor
antimicrobial use and resistance.2
In 2013, the Department of Health and the Department of Agriculture began to develop a ‘one health’ approach to resistance management, and released the National Antimicrobial Resistance Strategy in June 2015.3 One of the seven objectives was surveillance. The Australian Commission on Safety and Quality in Health Care was assigned the task of establishing this surveillance program, and set up the Antimicrobial Use and Resistance in Australia (AURA) project. The first national AURA report was released in June 2016.4
The Commission used a
structured approach to ensure that all relevant data in human health were
included. Both passive and targeted surveillance strategies were used to
capture data on antimicrobial use and resistance. The Commission identified
existing programs that were national or could become national:
The Commission reviewed these programs for
suitability and national coverage, and enhanced and expanded them where
necessary. This was largely achieved by the time the first national report was
prepared. The report was prepared along similar lines to those generated by the
benchmark countries in Scandinavia and the Netherlands, but also included data
on appropriate antimicrobial use. The benchmark countries do not currently
survey this.
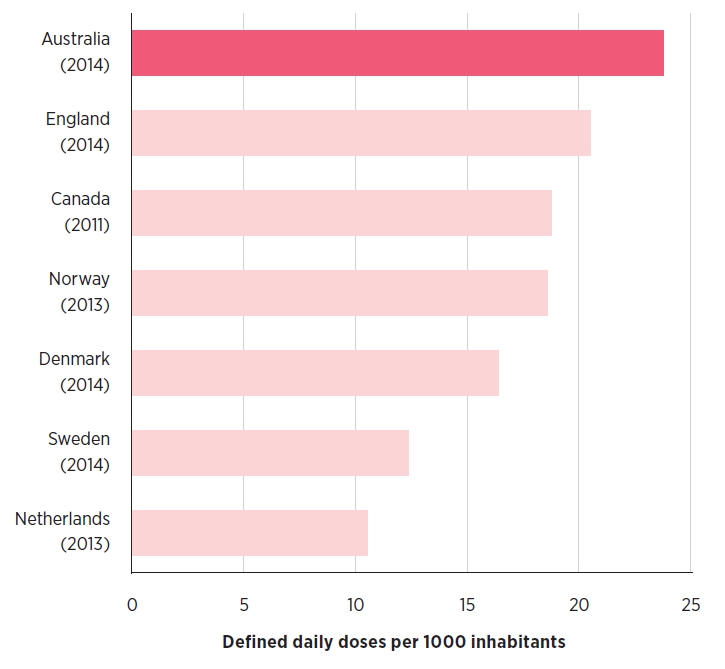
The first AURA report focuses primarily on
data from 2014, as this is the first year where complete data were available
from all programs.4 Historical data were included when they were
reliable and useful for interpretation. Where possible, comparisons with other
countries were made on overall antibiotic use and on key pathogens.
The main findings in antimicrobial resistance
data were:
The main findings on antimicrobial use were:
The AURA report collates valuable national information for the first time on antimicrobial use and resistance. Major areas for improvement in antimicrobial use have been identified in hospitals, residential aged care and especially in the community. The report provides baseline and some trend data on the resistances that are triggered by this use. The AURA program will continue to develop and refine its approach to national surveillance, and become a major part of the national strategy to contain antimicrobial resistance. It will provide the necessary data for monitoring the effects of interventions to reduce inappropriate use through stewardship and regulation, as described in the National Antimicrobial Resistance Strategy.3
Conflict of interest: none declared
Senior consultant, Australian Commission on Safety and Quality in Health Care, Sydney
