Abnormal laboratory results
Approach to the diagnosis of secondary hypertension in adults
- Ranita Siru, Johan H Conradie, Melissa J Gillett, Michael M Page
- Aust Prescr 2021;44:165-9
- 1 October 2021
- DOI: 10.18773/austprescr.2021.038
Corrected 18 August 2022. View correction.
This is the corrected version of the article.
Presentations that should raise suspicion of secondary hypertension include early-onset, severe or resistant hypertension. A suggestive family history or clinical clues can point to a specific secondary cause.
The most common causes and associations are renal disease, primary aldosteronism and obstructive sleep apnoea. Medicines, illicit substances and alcohol may also be responsible.
The assessment of patients begins with history taking and examination, to look for clinical clues. Laboratory tests include electrolytes, urea, creatinine and the aldosterone:renin ratio, urinalysis and the urine albumin:creatinine ratio. Abnormal results should prompt further investigation.
Initial testing for primary aldosteronism is best done before starting potentially interfering antihypertensive drugs. If the patient is already taking interfering antihypertensive drugs that cannot be stopped, the interpretation of the aldosterone:renin ratio must consider the presence of those drugs. Specialist advice can be sought if needed.
Secondary hypertension occurs in approximately 10% of adults with hypertension.1 There are many possible causes (Table 1). Identifying and treating the cause can potentially cure or markedly improve hypertension and reduce the associated cardiovascular risk.1,2
The history and examination may raise suspicion of secondary hypertension. It is important to remember that drugs can cause hypertension. Laboratory tests can help to identify other causes.
Table 1 - Laboratory tests in the initial investigation of secondary hypertension
|
Cause* |
Prevalence in unselected hypertensive patients |
Clinical clues |
Laboratory tests |
|
Renovascular disease† |
5% |
Acute worsening of renal function after starting an ACE inhibitor or angiotensin receptor antagonist, flash pulmonary oedema, early-onset hypertension in a female, abdominal bruit |
Electrolytes and creatinine with eGFR Urinalysis Urine albumin:creatinine ratio |
|
Renal parenchymal disease† |
1% |
Haematuria, proteinuria, history of recurrent urinary tract infections or obstruction, family history, polycystic kidneys, abdominal mass |
Electrolytes and creatinine with eGFR Urinalysis Urine albumin:creatinine ratio |
|
Primary aldosteronism |
8% |
Hypokalaemia |
Aldosterone:renin ratio |
|
Drugs, alcohol and other substances |
2% |
Drug history, NSAIDs, SNRIs, decongestants, oral contraceptives, bupropion, ciclosporin, tacrolimus, cocaine, amphetamines, caffeine, nicotine, alcohol, liquorice, some herbal supplements |
|
|
Cushing’s syndrome |
<1% |
Striae (purplish-red), proximal muscle wasting, easy bruising, thin skin, rapid weight gain, central adiposity, moon facies, buffalo hump, pathologic fracture, diabetes mellitus |
Late night salivary cortisol on two occasions Free cortisol in 24-hour urine on two occasions 1 mg overnight dexamethasone suppression test Measuring a morning or random serum cortisol is not recommended owing to a low sensitivity and specificity for Cushing’s syndrome |
|
Phaeochromocytoma/ paraganglioma |
<1% |
Paroxysms or ‘spells’: headache, palpitations, sweating, pallor, labile blood pressure |
Plasma metanephrines |
|
Aortic coarctation † |
<1% |
Well-developed upper body, hypertension confined to the upper limbs, systolic murmur |
|
|
Obstructive sleep apnoea ‡ |
25% |
Snoring, daytime somnolence, morning headache |
eGFR estimated glomerular filtration rate
NSAIDs non-steroidal anti-inflammatory drugs
SNRIs serotonin noradrenaline reuptake inhibitors
* Other rare causes of secondary hypertension include acromegaly, thyroid dysfunction and primary hyperparathyroidism.
† Laboratory tests should be complemented by imaging.
‡ Obstructive sleep apnoea has a very strong and important association, but may not be a cause of secondary hypertension.
International and local guidelines differ in their recommendations and prescriptiveness in relation to screening for secondary causes of hypertension. In general, patients with hypertension and any of the following characteristics should be screened:1,3
All patients suspected of having secondary hypertension should be screened for the common causes and associations. These include renal disease (parenchymal or renovascular), primary aldosteronism, medicines, illicit substances, alcohol and obstructive sleep apnoea. Other, less prevalent causes should only be investigated if there is strong clinical suspicion of a particular disorder, such as coarctation of the aorta. It is important to remember that a lack of adherence to antihypertensive treatment can cause persistent hypertension.
Patients with primary aldosteronism have a higher risk of cardiovascular morbidity and mortality than other age-, sex- and blood pressure-matched patients.3 Although testing for primary aldosteronism has not been directly linked with mortality benefits, treating primary aldosteronism surgically (by unilateral adrenalectomy) or with specific mineralocorticoid blockade may improve long-term cardiovascular outcomes.4
Hypertension is often the only sign of primary aldosteronism. Most patients do not present with the classical feature of hypokalaemia.
Screening for primary aldosteronism is straightforward if the patient has not started antihypertensive therapy. This involves a blood test, in an unfasted patient who has been ambulatory for at least two hours. It measures aldosterone and renin, allowing calculation of the aldosterone:renin ratio.3 This ratio is important as some patients with primary aldosteronism will have normal concentrations of aldosterone. As hypokalaemia can cause a false-negative ratio, potassium should be concurrently measured.
Reference intervals and screening thresholds for aldosterone, renin and their ratio vary according to the laboratory’s method of measurement (laboratories may measure either direct renin or plasma renin activity). The ratio should be interpreted in the context of the absolute values for aldosterone and renin. For example, a raised ratio due to a very high aldosterone with a non- suppressed renin concentration may be more suggestive of secondary hyperaldosteronism due to diuretic use or other causes. The ratio could also be raised because of a very low renin, even if the aldosterone concentration is not as high as is typically seen in primary aldosteronism.
The finding of an increased aldosterone:renin ratio not explained by interfering antihypertensives and confirmed on more than one occasion should prompt referral to a physician with an interest in hypertension, for consideration of confirmatory dynamic testing and specific treatment.
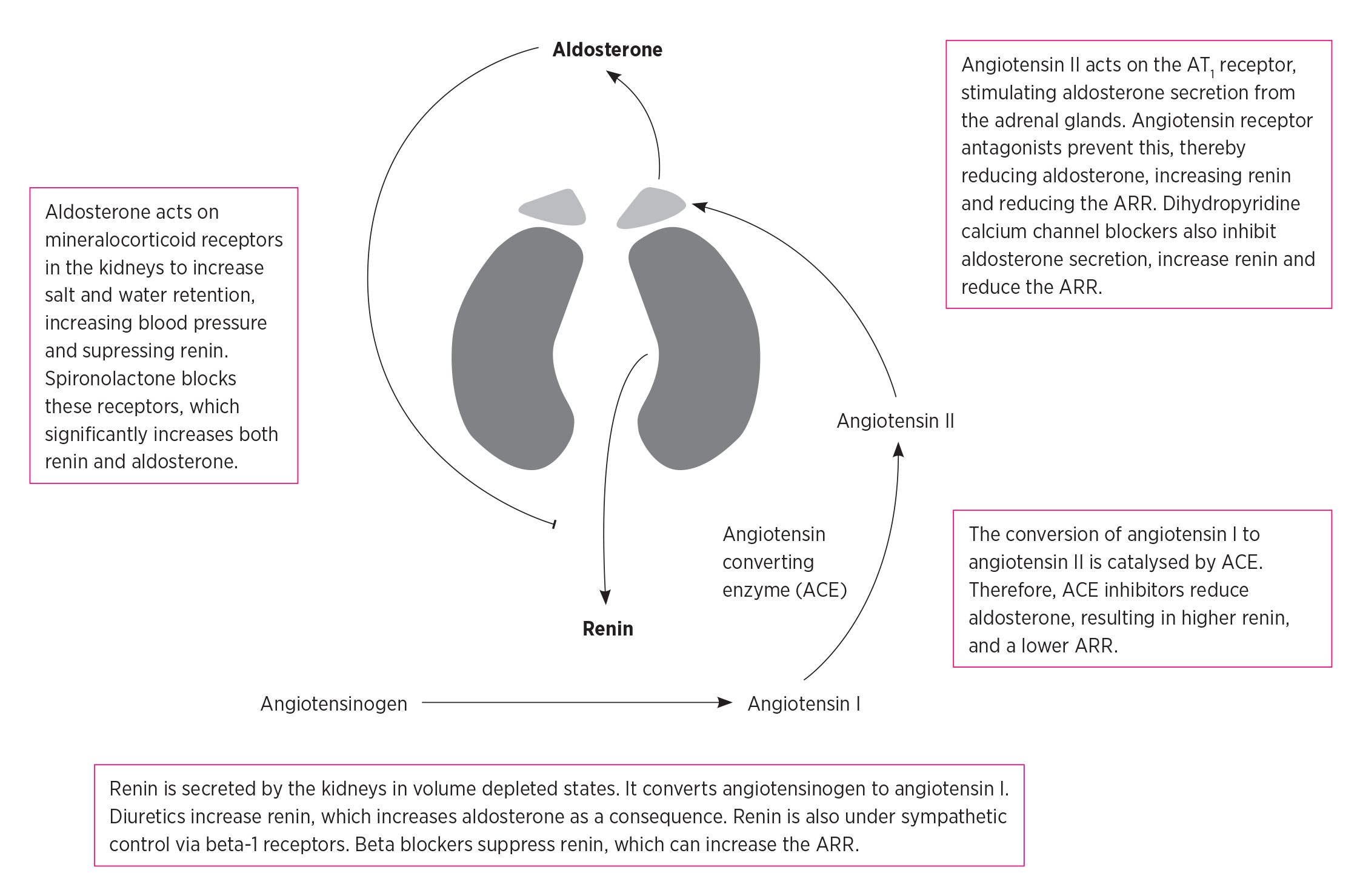
Although most antihypertensives affect the plasma concentrations of aldosterone, renin and their ratio (see Fig. and Table 2), additional indications may prevent the suspension of some drugs, such as when a beta blocker is also being used to control an arrhythmia. Initial testing therefore ofte needs to take place while the patient is still taking interfering antihypertensives. Interpreting an aldosterone:renin ratio while a patient is taking interfering antihypertensives can be difficult. Documenting the patient’s antihypertensive drugs on the request form will assist the pathologist’s analysis.
ARR aldosterone:renin ratio
Table 2 - Factors that may lead to false-positive or false-negative aldosterone:renin ratio results
|
Factor |
Effect on aldosterone plasma concentration |
Effect on renin concentration |
Effect on aldosterone:renin ratio |
|
Drugs* |
|||
|
Beta adrenergic blockers |
↓ |
↓↓ |
↑ (FP) |
|
Central agonists (e.g. clonidine, alpha methyldopa) |
↓ |
↓↓ |
↑ (FP) |
|
Non-steroidal anti-inflammatory drugs |
↓ |
↓↓ |
↑ (FP) |
|
Potassium wasting diuretics |
→ ↑ |
↑↑ |
↓ (FN) |
|
Potassium sparing diuretics |
↑ |
↑↑ |
↓ (FN) |
|
ACE inhibitors |
↓ |
↑↑ |
↓ (FN) |
|
Angiotensin receptor antagonist |
↓ |
↑↑ |
↓ (FN) |
|
Calcium channel blockers (dihydropyridines) |
→ ↓ |
↑ |
↓ (FN) |
|
Renin inhibitors |
↓ |
↓ ↑ |
↑ (FP) ↓ (FN) |
|
Potassium status |
|||
|
Hypokalaemia |
↓ |
→ ↑ |
↓ (FN) |
|
Potassium loading |
↑ |
→ ↓ |
↑ |
|
Dietary sodium |
|||
|
Sodium restriction |
↑ |
↑↑ |
↑ (FN) |
|
Sodium loading |
↓ |
↓↓ |
↑ (FP) |
|
Advancing age |
↓ |
↓↓ |
↑ (FP) |
|
Premenopausal women (vs males) † |
→ ↑ |
↓ |
↑ (FP) |
|
Other conditions |
|||
|
Renal impairment |
→ |
↓ |
↑ (FP) |
|
PHA-2 |
→ |
↓ |
↑ (FP) |
|
Pregnancy |
↑ |
↑↑ |
↓ (FN) |
|
Renovascular hypertension |
↑ |
↑↑ |
↓ (FN) |
|
Malignant hypertension |
↑ |
↑↑ |
↓ (FN) |
FN false negative, FP false positive
↓ decreases effect, ↑ increases effect, → has no effect
PHA-2 pseudohypoaldosteronism type 2 (familial hypertension and hyperkalaemia with normal glomerular filtration rate)
* Renin inhibitors lower plasma renin activity, but raise direct renin concentration. This would be expected to result in false-positive aldosterone:renin ratios for renin measured as plasma renin activity and false negatives for renin measured as direct renin concentration.
† In premenopausal, ovulating women, plasma aldosterone concentrations measured during the menses or the proliferative phase of the menstrual cycle are similar to those of men but rise briskly in the luteal phase. Because renin concentrations are lower, the aldosterone:renin ratio is higher than in men for all phases of the cycle, but especially during the luteal phase during which aldosterone rises to a greater extent than renin. False positives can occur during the luteal phase, but only if renin is measured as direct renin concentration and not plasma renin activity. In preliminary studies, some investigations have found false positives on the current cut-offs for women in the luteal phase. Accordingly, it would seem sensible to screen women at risk in the follicular phase, if practicable.
Source: adapted from reference 3
A suppressed renin, high aldosterone and raised ratio in a patient taking an ACE inhibitor alone (expected to increase renin and decrease aldosterone) would be suspicious for primary aldosteronism. However, a normal ratio in the same patient would not exclude primary aldosteronism, as it may be a false negative. On the other hand, beta blockers decrease renin concentrations. A patient taking a beta blocker who has a non-suppressed renin concentration probably does not have primary aldosteronism, but a suppressed renin and a raised ratio could be a false-positive result.
Sometimes, substitution of interfering antihypertensives with non-interfering antihypertensives is required to obtain a reliable ratio. This is also important for further confirmatory testing that may follow initial screening. Table 3 shows non-interfering antihypertensives that may be used during the workup to control blood pressure.5 As adjusting the antihypertensive regimen can be a lengthy process and is not without risks, it should only be pursued for patients expected to benefit from the diagnosis and treatment of primary aldosteronism. A discussion with a physician with a special interest in hypertension should be considered, and the patient should understand why changes to their treatment are being proposed.
Table 3 - Drugs that do not interfere with calculating the aldosterone:renin ratio5
|
Starting dose |
Maximum dose |
|
|
Sustained-release verapamil* |
180 mg daily |
240 mg daily |
|
Moxonidine |
200 micrograms once at night |
200 micrograms twice daily after two weeks |
|
Prazosin |
0.5 mg twice daily |
5 mg three times a day |
|
Hydralazine hydrochloride |
12.5 mg twice daily |
50 mg three times a day |
* Administration of verapamil as two divided doses may provide better coverage over 24 hours, if necessary. Doses higher than 240 mg daily may be used, but are often limited by adverse effects, therefore addition of a second drug is advised before increasing the verapamil dose.
When adjusting the antihypertensive regimen, drugs are usually ceased one at a time at a rate of one per week, or more slowly if there is a need to maintain blood pressure control. Diuretics including spironolactone are stopped first, as they require a washout of at least four weeks. Other antihypertensives need to be ceased for a minimum of two weeks before testing.3 Blood pressure should be monitored at least twice a week. Home blood pressure monitoring can be helpful for selected patients. Non-interfering antihypertensives, if required, may be introduced and up-titrated one at a time. The target blood pressure may be individualised based on the patient’s previous blood pressure, their age and the duration of hypertension. This blood pressure may be higher than the usual target for the prevention of cardiovascular disease, given that these drug substitutions are only temporary.
Patients should be informed of the symptoms of a hypertensive emergency, what a safe blood pressure is and how to seek medical attention if their blood pressure exceeds this. Provide counselling about the adverse effects, the frequency of dosing for the non-interfering antihypertensives, and the precautions for driving.
Identifying secondary hypertension presents an opportunity to modify a patient’s cardiovascular risk profile beyond what is achievable by antihypertensive therapy alone. Renal disease and primary aldosteronism are common causes.
A methodical approach to identifying the cause is necessary and must take into account the drugs being used by the patient. Advice on test selection and patient preparation to optimise the value of initial investigations can be provided by a chemical pathologist or hypertension specialist. Patients who have abnormal results will require further investigations to confirm the cause.
Conflicts of interest: none declared
This article is peer-reviewed.
Australian Prescriber welcomes Feedback.
Endocrinologist and Chemical pathology registrar, Department of Biochemistry, Western Diagnostic Pathology, Perth
Head of Biochemistry and Chemical pathologist, Department of Biochemistry, Western Diagnostic Pathology, Perth
Chemical pathologist and Endocrinologist, Department of Biochemistry, Western Diagnostic Pathology, Perth
Head of Biochemistry and Chemical pathologist, Department of Biochemistry, PathWest Laboratory Medicine, Fiona Stanley Hospital, Perth
Chemical pathologist, Department of Biochemistry, Western Diagnostic Pathology, Perth
