Article
Cluster headache in adults
- Jason C Ray, Richard J Stark, Elspeth J Hutton
- Aust Prescr 2022;45:15-20
- 1 February 2022
- DOI: 10.18773/austprescr.2022.004
Cluster headache is characterised by attacks of very severe, unilateral headache lasting 15–180 minutes, up to eight times per day. The attacks are associated with cranial autonomic symptoms on the same side and a sense of agitation or restlessness.
First-line acute abortive treatments include intranasal or subcutaneous sumatriptan or high-flow oxygen. Neuromodulation may benefit some patients.
First-line preventive therapy is high-dose verapamil. Close monitoring is required for the adverse effect of arrhythmia.
There are several emerging therapies that have either proven efficacy, or possible benefit for cluster headache. They include drugs aimed at the calcitonin gene-related peptide.
Cluster headache is a type of trigeminal autonomic cephalalgia. It is known colloquially as the ‘suicide headache’ because it is among the worst pains that can be experienced and many patients contemplate suicide during the attacks.1,2 Compounding the morbidity of the disease, there can be a significant delay in diagnosis of up to eight years, and therefore a delay in optimal treatment.3
The pooled lifetime prevalence of cluster headache is 0.12%. There is an overall male predominance of 4.3:1, which is higher in chronic cluster headache (15:1) than in episodic cluster headache (3.8:1).4 There is a significant genetic component with first-degree relatives having an 18 times higher risk of the disease.5 Attacks are triggered by the interplay of endogenous and exogenous factors such as alcohol and seasonal and diurnal variation. Smoking is a well-known risk factor in chronic cluster headache.6
Cluster headache accounts for 20% of headaches which always occur on the same side of the head (side-locked headache).7 When evaluating a patient, secondary causes of headache should first be considered and excluded. An anterior location of pain, sense of internal restlessness or agitation, and ipsilateral autonomic features (conjunctival injection, lacrimation, rhinorrhoea, eyelid oedema, sweating, miosis or ptosis) are highly suggestive of one of the trigeminal autonomic cephalalgias. The duration of pain and response to treatment helps differentiate these conditions (see Fig.).7
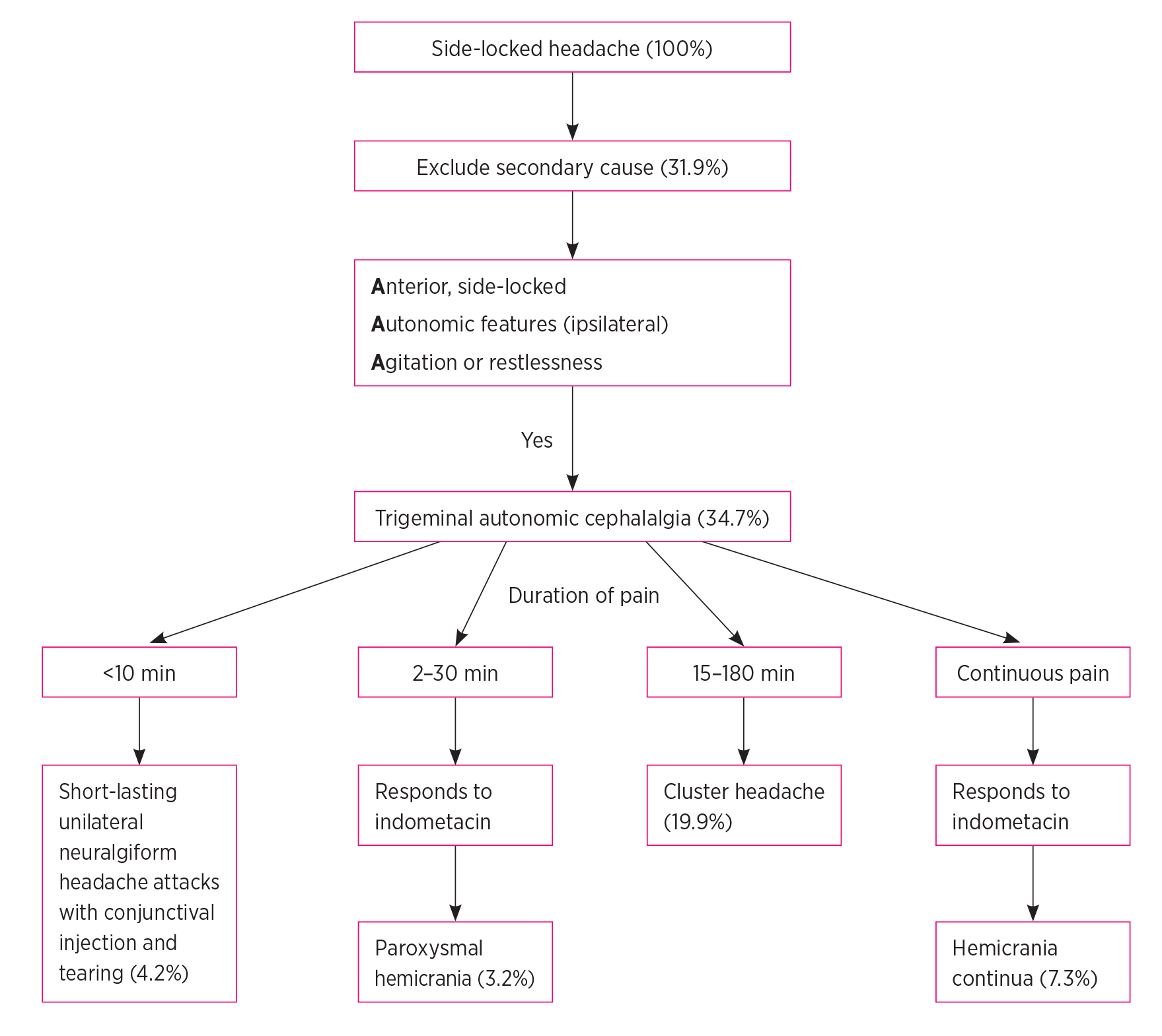
Cluster headaches are characterised by severe pain occurring over the orbit, supraorbital or temporal region lasting 15–180 minutes. They are associated with ipsilateral cranial autonomic features and a sense of internal restlessness or agitation (see Box).8 During cluster periods, cluster headache attacks occur up to eight times per day, typically at night.8 In episodic cluster headache the cluster periods last between seven days and one year and are separated by pain-free remission periods of three months or more. The 10–15% of patients who do not experience remission, or have a remission lasting less than three months, have chronic cluster headache.5,8 All patients presenting with cluster headache require MRI of the brain, including the pituitary region to exclude a secondary cause mimicking cluster headache (‘symptomatic cluster headache’). These include vascular causes, inflammatory pathology or a neoplasm.9
Paroxysmal hemicrania is another type of the trigeminal autonomic cephalalgia. The headache can be of similar duration to cluster headache, but there are more attacks (5–40/day) and no nocturnal emphasis. It responds to a trial of indometacin (25 mg three times a day then increasing, if there is no or only a partial effect, at three-day intervals to 50 mg, then 75 mg three times a day with gastric ulcer prophylaxis).10 The gastric ulcer prophylaxis is stopped when the indometacin is stopped.
The pathophysiology of cluster headache is not completely understood. With advances in clinical and neuroimaging studies, the vascular theory of cluster headache is now considered incomplete.11 There are vascular changes, but they are a consequence of neurological processes. While the precise mechanisms are still debated, recognition of three key structures involved in the pathophysiology aids in the understanding of the clinical features of the disease. These are the:
The trigeminocervical complex connects the peripheral trigeminal neurons to the central nervous system. Activation of the trigeminal system results in release of several neuropeptides including calcitonin gene-related peptide, a potent vasodilator, through activation of transient receptor potential cation subfamily V1 (TRPV1).5,13 As pain is perceived unilaterally in the ophthalmic division of the trigeminal nerve, the activation is theorised to be unilateral. However, this theory is unproven and the inefficacy of neurolysis of the trigeminal nerve serves as evidence that the origin of the perception of pain is incompletely understood.5,11
The trigeminal nerve connects through the superior salivatory nucleus to the parasympathetic fibres of the facial nerve, where they pass through the sphenopalatine ganglion. Activation of the parasympathetic system by the trigeminal nerve (termed the trigeminal autonomic reflex) is also responsible for the release of various neuropeptides including pituitary adenylate cyclase-activating polypeptide (PACAP)5 and ipsilateral cranial autonomic symptoms.
Functional imaging shows that the hypothalamus is involved in the circadian and circannual rhythmicity of cluster headache.14 The suprachiasmatic nucleus plays a critical role in circadian rhythm, and the nocturnal peak of melatonin is blunted in patients with cluster headache, however the significance of this is unclear.5
Management of cluster headache may be divided into acute abortive and preventive therapies, possibly with bridging therapy between them. The drugs used for the acute and preventive treatment of cluster headache are off label, but supported by clinical evidence. The majority of patients require preventive therapy, however patients with episodic cluster headache with seasonal bouts may only require abortive therapy, which provides symptomatic benefit but does not alter the cluster duration, or short-term prevention. Bridging therapies are frequently used at the start of a cluster to control attacks while up-titrating preventive therapy. During a bout of attacks, avoiding triggers such as alcohol, nitrate-containing foods and strong odours can be beneficial.15
First-line, evidence-based, abortive treatments for cluster headache include triptans and high-flow 100% oxygen through a well-fitting mask (Table 1).5,15-21 While several formulations of triptans have been studied in cluster headache, subcutaneous or intranasal preparations are recommended for their rapid onset of action. Triptans can be repeated after two hours. Although patients find both are helpful, there has been no head-to-head trial comparison of oxygen and subcutaneous sumatriptan.22 Oxygen, which is delivered via a non-rebreather mask and oxygen cylinder at 7–12 L/minute for 15 minutes, may be ordered from medical gas supply companies in Australia with a prescription.
Table 1 - Acute abortive therapies for cluster headache5,15-21
|
Therapy |
Dose |
Efficacy |
Possible mechanism of action |
|
Sumatriptan (subcutaneous) |
6 mg (12 mg) |
Mild or no pain at 15 min: 75% (32%) Pain-free at 15 min: 48% (17%) |
5-HT1B/D/F receptors – inhibit calcitonin gene-related peptide release and nociceptive signalling in trigeminocervical complex, and cause vasoconstriction of cerebral vessels which is possibly contributory |
|
Sumatriptan (intranasal) |
20 mg (40 mg) |
Mild or no pain at 30 min: 57% (26%) Pain-free at 30 min: 47% (18%) |
|
|
Zolmitriptan (intranasal)* |
5 mg (20 mg) |
Mild or no pain at 15 min: 15% (7%), at 30 min: 45% (30%) Pain-free at 15 min: 8% (3%), at 30 min: 32% (18%) |
|
|
Zolmitriptan (intranasal)* |
10 mg (20 mg) |
Mild or no pain at 15 min: 28% (7%), at 30 min: 62% (30%) Pain-free at 15 min: 12% (3%), at 30 min: 48% (18%) |
|
|
High-flow oxygen |
7–12 L/min for 15 min |
Reduction in pain at 15 min: 78% (20%) Pain-free at 15 min: 78% (20%) |
Vasoconstriction, blocks trigeminal autonomic reflex, inhibits protein release and activity in the superior salivatory nucleus |
|
Non-invasive vagal nerve stimulation (episodic cluster headache only) |
3 stimulations for 2 min |
Mild or no pain at 15 min: 39% (12%) |
Blocks trigeminal autonomic reflex, inhibits nociceptive signalling in trigeminocervical complex |
* Intranasal zolmitriptan is currently not available in Australia.
The choice of acute therapy depends on patient factors and cost. Oxygen is contraindicated in active smokers and patients with type 2 respiratory failure. Triptans are contraindicated in patients with ischaemic heart disease.
Other abortive treatments that have some supporting evidence in cluster headache include non- invasive stimulation of the vagal nerve.23 Trials are investigating other forms of neuromodulation..
Despite a lack of supportive randomised data, prednisolone is commonly used as a bridging preventive strategy to allow the up-titration of safer long-term preventive therapies. A variety of prednisolone regimens have been successful in uncontrolled studies, however prolonged use should be minimised because of its adverse effects. Starting at 1 mg/kg (maximum dose 75 mg daily) with gastric ulcer prophylaxis, and down-titrating over two weeks, is one reasonable strategy.15,16
An alternative strategy is a greater occipital nerve block with an injection of local anaesthetic and depot- methylprednisolone. This combination can reduce attacks for on average four weeks and avoids the adverse effects of a course of oral steroids.24
Preventive therapy may be indicated long term in patients with chronic cluster headache, or seasonally, in patients with episodic cluster headache, depending on their history. Immediate-release or controlled- release verapamil is first line, and its use is supported by a randomised controlled trial, in which 80% of patients had a halving of attack frequency and 26% were attack free.25 Its efficacy is dose-dependent and the doses required for disease control can be in excess of the usual dose. Specialists can sometimes use up to 960 mg per day in divided doses (Table 2).5,15,16 Patients therefore require ECG monitoring before starting verapamil, during titration, and even after reaching a stable dose. One in five patients will develop an arrhythmia and delayed-onset arrhythmias have been reported.26,27 Arrhythmias include first-degree heart block, second-degree heart block, junctional rhythms, right bundle branch block and bradycardia.26 There is a need to check for drug interactions. Once a bout of cluster headache has finished, the patient can be weaned cautiously off verapamil, by 80 mg every one to two weeks.
Table 2 - Preventive therapy for cluster headache5,15,16
|
Drug |
Dosing |
Monitoring |
Possible adverse effects |
Possible mechanism of action |
|
Verapamil (immediate-release formulation*) (Grade 1B) |
Start: 80 mg three times a day for at least 2 weeks Titrate: increase by 80 mg every 2 weeks Range: 240–960 mg |
ECG: before starting and at every dose change Repeat at stable dose after 10 days, every 1–2 months then every 6 months |
Constipation, peripheral oedema, bradycardia, conduction abnormalities. Cytochrome P450 3A4 inhibitor. There is a potential for drug interactions |
Voltage-gated calcium channels: decreases calcitonin gene-related peptide release, alters circadian rhythm |
|
Lithium (Grade 1B) |
Start: 300 mg daily for at least 1 week Titrate: increase by 300 mg every week Range: 300–1200 mg |
Monitor thyroid, kidney function, calcium, magnesium Monitor lithium concentration (initial aim 0.6–0.8 mmol/L) |
Include tremor, dizziness, dry mouth, weight gain, fatigue, anorexia, ataxia, gastrointestinal upset |
Alters glutamate, dopamine, gamma aminobutyric acid, circadian rhythm |
|
Galcanezumab (episodic) |
Start: 240 mg subcutaneous Continue: 120 mg every 4 weeks |
Not required |
Constipation, local injection site reaction, nasopharyngitis |
Inhibition of calcitonin gene-related peptide |
|
Topiramate (Grade 1B) |
Start: 25 mg daily for ≥1 week Titrate: increase by 25–50 mg/week Range: 100–200 mg |
Monitor kidney function |
Cognitive slowing, paraesthesia, kidney stones, gastrointestinal upset |
Inhibits trigeminal nociception, enhances gamma aminobutyric acid |
|
Melatonin (Grade 2C) |
Start: 4 mg daily for ≥1 week Titrate: increase by 4 mg every week Range: typically 8–10 mg, compounded |
Monitor sedation |
Drowsiness, gastrointestinal upset |
Alters circadian rhythm, enhances gamma aminobutyric acid |
* Controlled-release formulation may also be used with twice-daily dosing
Grade 1 strong recommendation
Grade 2 weak recommendation
Grade A high-level evidence
Grade B moderate-level evidence
Grade C low-level evidence
Lithium is considered second-line for the prevention of cluster headache. There are limited controlled data on its use, however in one trial it had similar efficacy to verapamil, but more adverse effects (29% vs 12%).28 The use of lithium is limited by its long-term adverse effects, toxicity and the need for strict monitoring.
Topiramate showed efficacy in a single open-label trial, but while it is a reasonable third-line option, cognitive adverse effects may limit its use.29 There is also weaker evidence for pizotifen and gabapentin, and conflicting evidence for melatonin and valproate. They are generally used as adjuvant therapies to other preventive drugs.5,15,30
Several invasive and non-invasive neuromodulatory techniques have been investigated in cluster headache. Electrical stimulation of the sphenopalatine ganglion, occipital nerve and vagal nerve have all been effective at reducing attack frequency. However, these procedures are reserved for drug-refractory cluster headache due to the need for surgery, their cost and the risk of complications.5 Access to invasive neuromodulatory techniques in Australia is limited.
Neuromodulation can be highly effective in select groups. In a randomised controlled trial of sphenopalatine ganglion neurostimulation (involving implantation of a device not available in Australia) for refractory cluster headache, 67% of patients achieved pain relief.31 Other trials studied radiofrequency ablation of the sphenopalatine ganglion. In the largest case series of 66 patients there was pain relief in 60% of those with episodic cluster headache and in 30% of those with chronic cluster headache.31,32
A phase III trial of occipital nerve stimulation has been completed. It compared low- (30%) and high-intensity (100%) stimulation for refractory chronic cluster headache. Overall, the median weekly mean attack frequency reduced to 7.4. The reduction was greater in the high-stimulation group. However, the difference between the groups was –2.42 (95% confidence interval –5.17 to 3.33). Serious adverse events, such as pain, were reported in 26% of the high-stimulation and 12% of the low-stimulation groups.33
Non-invasive stimulation of the vagus nerve has been studied for acute treatment of cluster headache in two randomised, sham-controlled trials. There was a significant response in episodic cluster headache, but not chronic cluster headache.34,35 In one trial of non-invasive stimulation of the vagus nerve for prevention, the number of weekly attacks reduced by 5.9 compared to 2.1 with sham treatment.36
Galcanezumab is a monoclonal antibody against calcitonin gene-related peptide. In episodic cluster headache galcanezumab reduced weekly attacks by 71%. Fremanezumab, another calcitonin gene-related peptide monoclonal antibody, was not effective in episodic cluster headache. Neither drug was effective for chronic cluster headache.37 This may have been due to poor trial design and differing neurobiology between episodic cluster headache and chronic cluster headache.37,38 Trials of eptinezumab, an intravenous calcitonin gene-related peptide monoclonal antibody, in episodic cluster headache are ongoing (NCT04688775).
Three prospective studies of onabotulinum toxin A using a variety of protocols have provided low-quality evidence that it may reduce attack frequency in cluster headache by up to 50%.39 A phase I–II trial of onabotulinum toxin A injected towards the otic ganglia found it to be safe in chronic cluster headache, but there was no significant reduction in attack frequency.40 A phase III trial is studying injections towards the sphenopalatine ganglion (NCT03944876).
Early specialist referral and co-management are recommended if there is any diagnostic uncertainty about the condition. A suboptimal response to management or a need for second- or third-line treatments are also indications for referral.
A cluster headache is one of the most excruciating pains imaginable. Recognising the condition and empowering patients with a plan for managing acute attacks and bridging therapies while titrating preventive therapy is key to limiting the morbidity of the disease.
Conflicts of interest: Jason Ray has received compensation from the Pharmaceutical Society of Australia, sponsored by Viatris for educational material.
Richard Stark has served on advisory boards for Novartis, Teva, Eli Lilly, Allergan, Lundbeck and has received payment for educational presentations from Allergan, Teva, Eli Lilly and Novartis.
Elspeth Hutton has served on advisory boards for Sanofi-Genzyme, Novartis, Teva, Eli Lilly, Allergan, Lundbeck, been involved in clinical trials sponsored by Novartis, Teva, Xalud, Daewong and Novotech, and has received payment for educational presentations from Allergan, Teva, Eli Lilly and Novartis.
This article is peer-reviewed.
Australian Prescriber welcomes Feedback.
Neurologist, Department of Neurology, Alfred Hospital, Melbourne
Neurologist, Department of Neurology, Austin Health, Melbourne
Headache fellow, Department of Neuroscience, Monash University, Melbourne
Neurologist, Department of Neurology, Alfred Hospital, Melbourne
Adjunct clinical associate professor, Department of Neuroscience, Monash University, Melbourne
Deputy director and Neurologist, Department of Neurology, Alfred Hospital, Melbourne
Head, Headache Service, Department of Neurology, Alfred Hospital, Melbourne
Head, Peripheral Neuropathy, Pain and Headache Group, Department of Neuroscience, Monash University, Melbourne


