Diagnostic tests
Current clinical applications of positron emission tomography
- Aravind Ravi Kumar
- Aust Prescr 2008;31:123-8
- 1 October 2008
- DOI: 10.18773/austprescr.2008.071
Positron emission tomography (PET) allows diagnostic imaging of metabolic function using radioisotopes. This technology has undergone significant growth and evolution in recent years with most PET scanners now integrated with CT scanners. The main radiotracer in clinical use is F-18 fluorodeoxyglucose. This was initially used as a research tool and in cardiac and neurological applications, but now has an integral role in oncology. Fluorodeoxyglucose PET has had a major impact on the management of a broad range of malignancies because it is more sensitive than conventional imaging modalities. It is now used for diagnosis, staging and assessing response to therapy in many cancers and in characterising solitary pulmonary nodules. It is important to remember that not all abnormalities on a fluorodeoxyglucose PET scan are due to malignancy, and unexpected findings may need to be evaluated further.
Positron emission tomography (PET) scanning allows non-invasive diagnostic imaging of metabolic processes using short-lived radioisotopes. In contrast to computerised tomography (CT) and magnetic resonance imaging (MRI), which provide information on structure, PET can quantify biochemical and physiological function.
PET has been available as a clinical tool in Australia for well over a decade. While initial clinical applications were largely in cardiology and neurology, these have been dwarfed by oncology indications, which now account for over 90% of PET scans worldwide. Facilities have been installed in every mainland state capital city and in Newcastle, New South Wales. At present, only specialists and consultant physicians may refer patients for a PET scan.
A significant recent advance has been hardware integration of CT scanners with PET scanners (PET CT), allowing one to obtain a synergistic combination of anatomical (CT) and functional information (PET) at the same time. Problems of patient and organ motion are also significantly reduced with this approach. Almost all sales of new PET scanners worldwide are now PET CT.
Radiotracers manufactured from positron emitting isotopes can be used to image a variety of biological processes in the body using a PET scanner. A positron is a positively charged electron which is emitted from the nucleus of some low molecular weight radioactive isotopes. These include carbon (C-11), nitrogen (N-13) and oxygen (O-18), which are the 'building blocks' of the body, and fluorine (F-18). These isotopes have very short half-lives (ranging from two minutes for O-18 to 110 minutes for F-18), and have to be manufactured nearby in a medical cyclotron. These isotopes can then be chemically incorporated into trace quantities of biologically relevant molecules. The radiotracers have no pharmacological actions.
A PET scanner does not directly image positrons. Once a positron is emitted from the nucleus, it travels a short distance (several millimetres in soft tissue), and then annihilates with a negatively charged electron. The mass of the two particles is converted to energy in the form of two gamma rays that propagate at 180o to each other. Coincident gamma ray pairs that travel out of the body are detected by a ring of detectors around the patient. Many millions of such 'events' are used to determine the distribution of radiotracers within the body.
In practice, the resolution of a modern PET scanner is 8–10 mm. A negative PET scan in lesions smaller than this cannot reliably exclude serious pathology. Lesions below this size however may still be detected on PET if they are very metabolically active.
The most commonly used radiotracer in clinical practice is F-18 fluorodeoxyglucose (FDG), a glucose analogue. Increased glucose metabolism is a characteristic feature of many malignant tissues. FDG-PET scans have been shown to be more accurate than conventional imaging in the evaluation of many (but not all) malignancies.
FDG is transported inside cells by the glucose transporter GLUT 1. The FDG molecule is then phosphorylated to FDG-6-phosphate by hexokinase. Further downstream glycolysis is not possible so the tracer is trapped in the cell in virtually all tissues.
No significant adverse reactions have yet been recorded from the intravenous injection of FDG in patients worldwide.
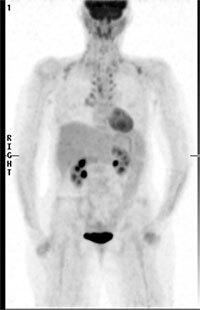
The brain is an obligate glucose user, and there is marked FDG uptake in normal cortex and deep nuclei. Cardiac FDG uptake is very variable as cardiac muscle switches between glucose and fatty acid metabolism depending on the fasting state. The liver demonstrates diffuse moderate levels of FDG uptake. Unlike glucose, there is significant FDG excretion by the kidneys into the bladder (Fig. 1).
A semi-quantitative measure of FDG uptake, the standardised uptake value (SUV), is quoted widely in the literature and is used by some centres in clinical reporting. Higher SUVs are more likely to be associated with malignancy and may be a marker of adverse prognosis. However, there is no 'cutoff' SUV that can distinguish between benign or malignant aetiologies. There may also be variability in SUV measurements and methodology between centres, so using SUV for comparing studies performed at different sites may be problematic.
A 4–6 hour fast is recommended for a standard FDG-PET oncology study to reduce cardiac and skeletal muscle FDG uptake. Extra preparation for diabetic patients includes avoiding insulin injections for at least four hours before the scan as insulin drives FDG into skeletal muscle. A blood sugar level of over 12 mmol/L can competitively inhibit tumour FDG uptake. In this instance the scan may be rescheduled.
Following standard preparation, the radiotracer is injected intravenously as a bolus (< 1 mL) and allowed to distribute in the body while the patient is lying comfortably in a quiet room for around 60 minutes. It is important that the patient is relaxed and still during the 'uptake phase' because actions such as talking, chewing gum and jaw clenching all cause FDG uptake in the relevant muscles and may sometimes obscure pathology.
Claustrophobia is rarely a contraindication (unlike MRI), but oral benzodiazepines may be used as an anxiolytic and to reduce FDG uptake in neck muscle during the uptake phase.
The use of oral and intravenous CT contrast agents is controversial as these may cause image artefacts on the PET scan. The PET scan itself takes around 20 minutes and typically ranges from skull base to thighs.
The radiation dose to the patient from a PET scan is around 8 milliSieverts (mSv). The CT component of the procedure varies, but most centres in Australia use a 'low-dose' non-contrast protocol which adds around 4 mSv. The total dose of 12 mSv is equivalent to around five years of normal background radiation, and is similar to a diagnostic CT scan of the same body region.
Although FDG is not excreted in breast milk, it is prudent to advise suspension of breastfeeding for six hours. No other special precautions need to be taken for the patient's relatives or carers due to the rapid decay of PET radiotracers.
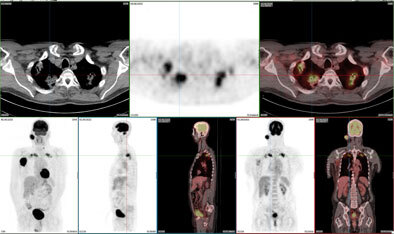
Medicare Australia-approved indications for FDG-PET are summarised in Table 1. It is important to emphasise that FDG-PET is not a 'cancer scan'. It shows areas of abnormal glucose metabolism. Non-malignant causes of FDG uptake are relatively common and should always be considered in the differential diagnosis (Fig. 1). Clinically implausible or unexpected abnormalities may require further confirmatory investigation. There are innumerable causes of FDG uptake that are not due to malignancy. Many of these can be recognised on correlation with patient history/physical examination or typical imaging patterns. Common causes are infection (including tuberculosis – see Fig. 2), inflammation (sarcoidosis and granulomatous diseases), trauma, enthesopathies and fractures.
|
||||||||
FDG-PET (and PET CT) has been shown to be more accurate than conventional imaging in a variety of malignancies in many clinical settings (for example staging, restaging, detection of occult primary site, rising tumour markers, assessment of residual mass, detecting radionecrosis from viable tumour). It is also cost-effective as PET often leads to upstaging of disease, thus reducing futile attempts at curative therapies, and helping allocation of finite resources to patients most likely to actually benefit from aggressive intervention.
Malignancies that typically have very high levels of FDG uptake include squamous cell carcinomas of the head and neck, oesophagus, most lung cancers, melanoma, most types of lymphoma, high-grade sarcoma and metastatic colon carcinoma. Gastric, uterine, cervical, breast, testicular and thyroid malignancies may also be usefully evaluated, but not all are reimbursed by Medicare (see Table 1).
Primary liver tumours generally have low FDG uptake (due to intracellular dephosphorylation of FDG) and may not be distinguishable from normal background liver, but liver metastases are sensitive to imaging. Other malignancies where FDG-PET is not useful (high false negative rate) include bronchoalveolar cell carcinoma of the lung, carcinoid tumours, mucinous adenocarcinomas and some low-grade sarcomas.
Malignancies of the urinary tract (such as renal cell, transitional cell and prostate carcinomas) are not well imaged due to variable FDG uptake in the tumours and high background levels of FDG in urine.
FDG-PET is not sensitive in detecting cerebral metastases because there is a high background uptake and the brain is not routinely included in the imaging field. However, FDG-PET may be indicated in the evaluation of primary brain tumours.
Bony metastases that cause densely sclerotic reaction (typically prostate cancer) are best imaged with bone scans as these lesions may be poorly FDG-avid. FDG-PET is much more sensitive for lytic, soft tissue or marrow lesions.
|
||||||||||||||||||||||||||||||||
Historically, the five-year survival rate after surgery of even clinical stage I lung cancer is only 50%, with much of the mortality being accounted for by undetected metastatic disease.
FDG-PET has an important role in staging and treatment planning in non-small cell lung cancer. Studies have shown that a staging PET scan predicts patient prognosis and mortality much more accurately than conventional imaging techniques.
FDG-PET detects unsuspected metastatic disease in 10–20% of patients, with a higher yield in patients with more clinically advanced disease. Confirmation of metastatic disease leads to decreased iatrogenic morbidity from fewer futile thoracotomies.
FDG-PET is the most accurate non-invasive means of mediastinal nodal staging, with a pooled sensitivity and specificity of 74% and 85%.1Its particular strengths are identifying benign (hyperplastic) but enlarged lymph nodes and to a lesser extent detection of metastatic disease in small sub-centimetre nodes. However, biopsy is still considered the gold standard. FDG-PET positive nodes should be confirmed by biopsy as they may be due to inflammation. Micrometastatic disease cannot be detected by any current non-invasive imaging technique.
External beam radiation therapy is also commonly used in the management of lung cancer. There is increasing interest in incorporating metabolic data from PET scans into radiotherapy planning systems, leading to PET-guided changes in radiotherapy fields. Clinical trial results of patient outcomes with this approach are currently sparse.
Pulmonary nodules are becoming an increasingly common diagnostic problem with more widespread use of CT scanning. No evaluation is complete without clinical risk factor assessment. Many pulmonary nodules cannot be characterised on CT, and may be difficult to biopsy. For lesions greater than 8–10 mm in size, FDG-PET has been shown to differentiate between benign and malignant nodules (sensitivity 87%, specificity 83%)2 and decreases the biopsy rate of benign lesions.
Lesions that are hypermetabolic should be considered malignant until proven otherwise. Granulomatous disease and infections are also hypermetabolic conditions and may be considered 'false positive' for malignancy, although they require specific diagnosis and treatment in their own right.
While complete absence of FDG uptake indicates a benign lesion, low levels of FDG uptake can be seen in carcinoid, bronchoalveolar and well differentiated adenocarcinomas. Stability on serial anatomical imaging over a two-year period is also considered an indicator that a lesion is benign.
Accurate staging is integral to the development of a management plan for most types of lymphoma. FDG-PET has superseded gallium scans in functional evaluation of both Hodgkin's and non-Hodgkin's lymphoma, and is considered the most accurate imaging test for this condition.
Overall, FDG-PET is more sensitive than CT scan in detecting extranodal (particularly marrow, liver and spleen – see Fig. 3) and small volume nodal involvement, and changes management during initial staging in a median of 10.5% of cases.3There is often variation between studies and pooled statistical data due to the many different histological subtypes, therapies and grades of biological behaviour of Hodgkin's and in particular non-Hodgkin's lymphoma.
Some lymphoma subtypes have variable or low FDG uptake including mucosa-associated lymphoid tissue (MALT)-type, small lymphocytic and marginal-zone lymphoma.

|
There is great interest in early prediction of response to chemotherapy. Identification of poor responders would lead to early change to second-line therapies, and there is potential to truncate therapy in good responders. The latter is particularly relevant in young patients with Hodgkin's disease where there are significant delayed toxicities from curative therapy. Prospective trials, particularly those in which truncation of therapy is guided by PET scan response, are still lacking.4
Studies also suggest that persistently positive PET scans several cycles into therapy implies the presence of chemotherapy resistant clones and therefore a worse prognosis.
Post-therapy FDG-PET scans can show a variety of features including diffuse skeletal uptake from bone marrow hyperplasia (particularly in the setting of colony stimulating factor use), thymic hyperplasia in younger patients, and inflammatory FDG uptake in recently irradiated tissues. The scan should therefore ideally be scheduled just prior to commencing the next cycle of therapy, or at least eight weeks after the completion of radiotherapy.
Assessment of remission status with CT is often uncertain due to the presence of residual masses after therapy, which may represent inactive scar tissue or residual active malignancy. PET (and PET CT) is considered the most accurate method of assessing this, with radiotherapy or further chemotherapy being considered for patients with active disease. Persistent FDG uptake in a residual mass is also an adverse prognostic marker.
Metastatic disease confined to liver or lung is now treated with surgical resection as a potentially curative procedure. FDG-PET aids greatly in patient selection by identifying sites of occult disease that would preclude surgery.
Analogous to lymphoma, FDG-PET is accurate in determining the aetiology of residual pelvic masses after therapy, and also has a role in the setting of rising carcinoembryonic antigen (CEA) with normal CT or MRI.
FDG-PET is not useful in the detection or primary staging of colon cancer due to the extremely variable physiological colonic uptake patterns. The exception to this is rectal cancer, where detection of nodal disease may influence neoadjuvant radiation or chemotherapy before definitive surgery.
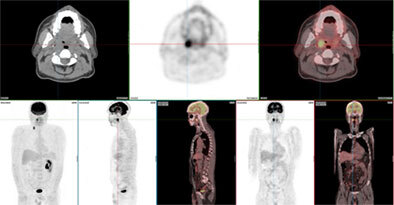
The site of an otherwise occult primary malignancy can be identified on PET in 25% of cases of metastatic head and neck squamous carcinoma (Fig. 4). FDG-PET is also used in post-therapy evaluation of head and neck cancer, where residual disease and sequelae of treatment may be difficult to distinguish on CT scan. A negative PET scan in this setting has a high negative predictive value but should only be performed at least 8–12 weeks after completion of therapy to avoid false positive results from residual inflammation.5
FDG-PET is useful for biopsy guidance in a variety of conditions, particularly soft tissue sarcomas which may have histological heterogeneity, and in larger necrotic masses to identify sites of viable tumour. Other indications for which PET is used include distinguishing radionecrosis from residual tumour in brain malignancies, and planning radiation therapy fields.
|
||||||||
Significant incidental findings are noted in up to 3% of scans, and often are an indicator of occult synchronous malignancies. Many malignancies also share common risk factors, particularly in head and neck, lung and upper gastrointestinal tract tumours in smokers. Other 'incidental' findings of particular significance that should not be ignored are FDG-avid thyroid nodules and focal uptake in the large bowel, which are associated with around a 25% risk of malignancy.
Future applications of PET are likely to come from tracers other than FDG. Non-oncology applications are also emerging, particularly in the fields of dementia, movement disorders and detection of infection.
A variety of tracers are under development and have undergone clinical trials. They include oncology applications as diverse as the imaging of tumour hypoxia, cellular proliferation, lipid membrane synthesis, receptor expression (for example, oestrogen receptor expression) and angiogenesis. These emerging 'molecular imaging' techniques may lead to new insights into disease biology, and play a central role in selection and monitoring of therapy.
Acknowledgement: Dr David Macfarlane, Director, Queensland PET Service, for his support and editorial assistance.
Staff specialist, Department of Nuclear Medicine and Queensland PET Service, Royal Brisbane and Women's Hospital, Brisbane