Article
Diabetes and periodontitis
- Robert Hirsch
- Aust Prescr 2004;27:36-8
- 1 March 2004
- DOI: 10.18773/austprescr.2004.035
Chronic gingivitis and periodontitis are common inflammatory conditions of the periodontal tissues. Given the 'right' concurrence of risk factors, a person with periodontitis can experience significant destruction of tooth-supporting bone, ultimately resulting in tooth loss. Poorly controlled diabetes is an important risk factor for periodontitis, and gingivitis and periodontitis are sometimes the first sign that a patient has diabetes. As severe periodontitis can lead to the loss of teeth, it is important that patients with diabetes practise good oral hygiene and have regular dental check-ups so that problems can be detected quickly.
In chronic periodontitis, the tooth supporting structures (alveolar bone and the periodontal ligament) are destroyed. The disease has a multi factorial origin. Complexes of commensal oral anaerobic bacteria and perhaps viruses are thought to interact with risk factors, such as smoking, diabetes and depression, to create the conditions which make a person susceptible to periodontitis. The patient's immuno-inflammatory response to the bacteria causes the tissue destruction which occurs in chronic periodontitis. Less than 5% of Australians are susceptible to the severe periodontitis which results in tooth loss, although up to 10% experience moderate amounts of periodontitis-related bone loss.
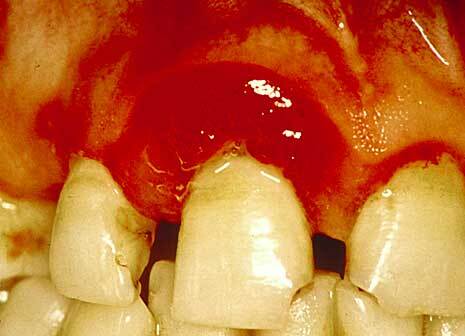
It is useful to distinguish chronic gingivitis from periodontitis. Chronic gingivitis is the very common inflammatory reaction occurring in the gingival tissues in response to the accumulation of dental plaque. It usually precedes the development of periodontitis, but chronic gingivitis does not inevitably progress to periodontitis. The clinical appearance of gingivitis may be modified by systemic factors such as poorly controlled diabetes, which can significantly accentuate the gingival tissues' response to dental plaque (Fig. 1)
Although periodontitis is a recognised complication of diabetes, people with well-controlled diabetes who have good oral hygiene are not at increased risk of periodontitis. However, their susceptibility to periodontitis is significantly increased when their diabetes is poorly controlled, particularly if they also smoke.
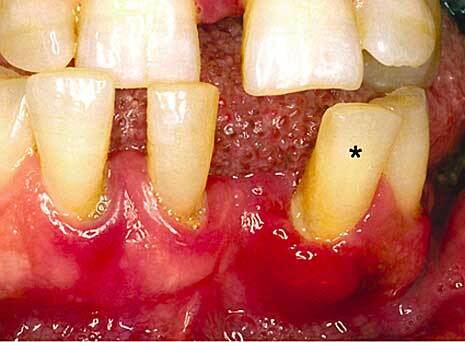
Recent epidemiologic evidence shows that the prevalence of diabetes in patients with periodontitis is significantly greater (by two times) than in people without periodontitis.1Given that diabetes may be present for a number of years before it is diagnosed, and that the prevalence of diabetes is increasing in the Australian community, dentists may be the first health professionals to detect a patient's diabetes. The gingival and periodontal signs which may alert the clinician that the patient has previously undiagnosed diabetes or that the patient's diabetes is poorly controlled, include:
|
|
|
Advanced glycation end products deposited in the tissues as a result of hyperglycaemia can alter the phenotype of macrophages and other cells via a specific cell-surface receptor. Macrophages are key cells in the pathogenesis of periodontitis through their ability to produce a large array of cytokines. They also influence the inflammatory response, the metabolism of fibroblasts and lymphocytes and stimulate bone resorption via prostaglandin E2. It is thought that the advanced glycation end products transform the macrophages into cells with a destructive phenotype, producing pro-inflammatory cytokines in an uncontrolled fashion.3
Neutrophils are the primary defence cells of the periodontium. The reduced neutrophil function observed in patients with diabetes is therefore another mechanism increasing the susceptibility to periodontitis.
While periodontitis is a recognised complication of poorly controlled diabetes, it has been proposed that severe periodontitis may make the metabolic control of diabetes more difficult. The process may be mediated through the systemic release of inflammatory cytokines (e.g. TNF-a) from periodontitis lesions, and chronic, low-level systemic exposure to Gram negative organisms. Although early studies have been poorly designed, one of these suggested that when antibiotics were added to standard periodontal treatment (debridement of the teeth and oral hygiene improvement), diabetic control improved significantly for a period of three months.2
People with diabetes need to practise high standards of daily oral hygiene, including brushing and flossing. The use of interdental brushes (which are like small bottle brushes) is indicated where there has been some recession of the gingivae. Adjunctive use of a chlorhexidine mouthwash (0.12%) or chlorhexidine gel (0.2%) twice daily (used independently of toothpaste so that the chlorhexidine is not inactivated) may be useful in controlling the more severe forms of gingivitis. Patients should consult with their dentist or periodontist regarding the recommended duration of use of chlorhexidine. Dental care, which is specifically aimed at monitoring the health of the periodontal tissues and providing the necessary treatment, is needed at six-month intervals.
Medical practitioners who suspect a patient has diabetes-related gingivitis or periodontitis should ensure that an early referral is made to a dentist. Dentists in turn need to refer advanced or suspect cases to a periodontist.
Medical and dental practitioners need to be aware of the interrelationship between poorly controlled or undiagnosed diabetes mellitus and chronic gingivitis and periodontitis. This is particularly important because of the rising prevalence of diabetes in the Australian community.
Conflict of interest: none declared
Photographs courtesy of the author
The following statements are either true or false.
Click anywhere on the panel for the answers.
1. Periodontitis may be the first presentation of diabetes.
2. Gingivitis precedes periodontitis.larly important because of the rising prevalence of diabetes in the Australian community.
Senior Lecturer, Dental School, The University of Adelaide, Adelaide