Diagnostic tests
Investigating thyroid nodules
- Nisha Venkatesh, Jui T Ho
- Aust Prescr 2021;44:200-4
- 1 December 2021
- DOI: 10.18773/austprescr.2021.055
Thyroid nodules are common clinically and even more common as an incidental finding during ultrasonography. Routine screening of thyroid nodules in patients with hyperthyroidism or hypothyroidism without risk factors for thyroid cancer is not recommended.
Most thyroid nodules are benign. Sonographic risk-stratification systems should be used to estimate the risk of malignancy and the need for fine-needle aspiration biopsy.
Malignant thyroid nodules require surgical management. Most thyroid cancers are well-differentiated papillary or follicular thyroid neoplasms, which have an excellent prognosis with a low mortality rate.
Clinically apparent thyroid nodules are present in approximately 5% of the adult population. In contrast, a far greater number of individuals are found to have incidental thyroid nodules on imaging performed for indications unrelated to the thyroid. Up to 68% of asymptomatic individuals without a history of thyroid disease who have undergone a screening thyroid ultrasound have been found to have a thyroid nodule ranging in size from a few millimetres to more than 1 cm.1 Nodules are more common in women, the elderly and in areas of iodine deficiency.2,3 Patients and doctors are often concerned that the nodules could be malignant.
Only 5–13% of nodules harbour thyroid cancers.4 Factors that increase the risk of malignancy are shown in the Box. Nodules that harbour thyroid cancer are often asymptomatic.
Worldwide, the incidence of thyroid cancer has been rising over the last few decades, reflecting the increasing use of medical imaging. However, the mortality has not risen significantly. In Australia it is estimated that 73% of thyroid cancer diagnoses in 2012 represented overdiagnoses. These individuals would never have developed symptomatic thyroid cancer in their lifetime.5
Well-differentiated thyroid neoplasms arise from follicular cells. These papillary and follicular carcinomas account for more than 90% of all cases.2 Medullary and anaplastic thyroid cancers are rare.6,7
Differentiated thyroid cancer has an excellent prognosis. Despite the presence of lymph node metastases in 5–20% of patients and distant metastases in 10–15%, the 10-year survival is 80–95%.8 This low mortality rate is supported by the incidental finding of differentiated thyroid cancer at autopsy in approximately 10% of individuals who died from other causes and did not have a history of thyroid disease.9
Given the high prevalence of incidental thyroid nodules and the low prevalence of thyroid cancers, some of which may never become clinically relevant within the individual’s lifetime, routine screening for thyroid nodules is not recommended in people without risk factors for thyroid cancer.10,11 In people with a detected thyroid nodule, a stepwise approach is required to determine whether the nodule is hyperfunctioning and whether it is malignant (Fig.).
The presence of multiple thyroid nodules or a multinodular goitre does not increase the risk of thyroid cancer. The recommended approach is to assess each nodule separately for the presence of high-risk sonographic features that would suggest malignancy.2
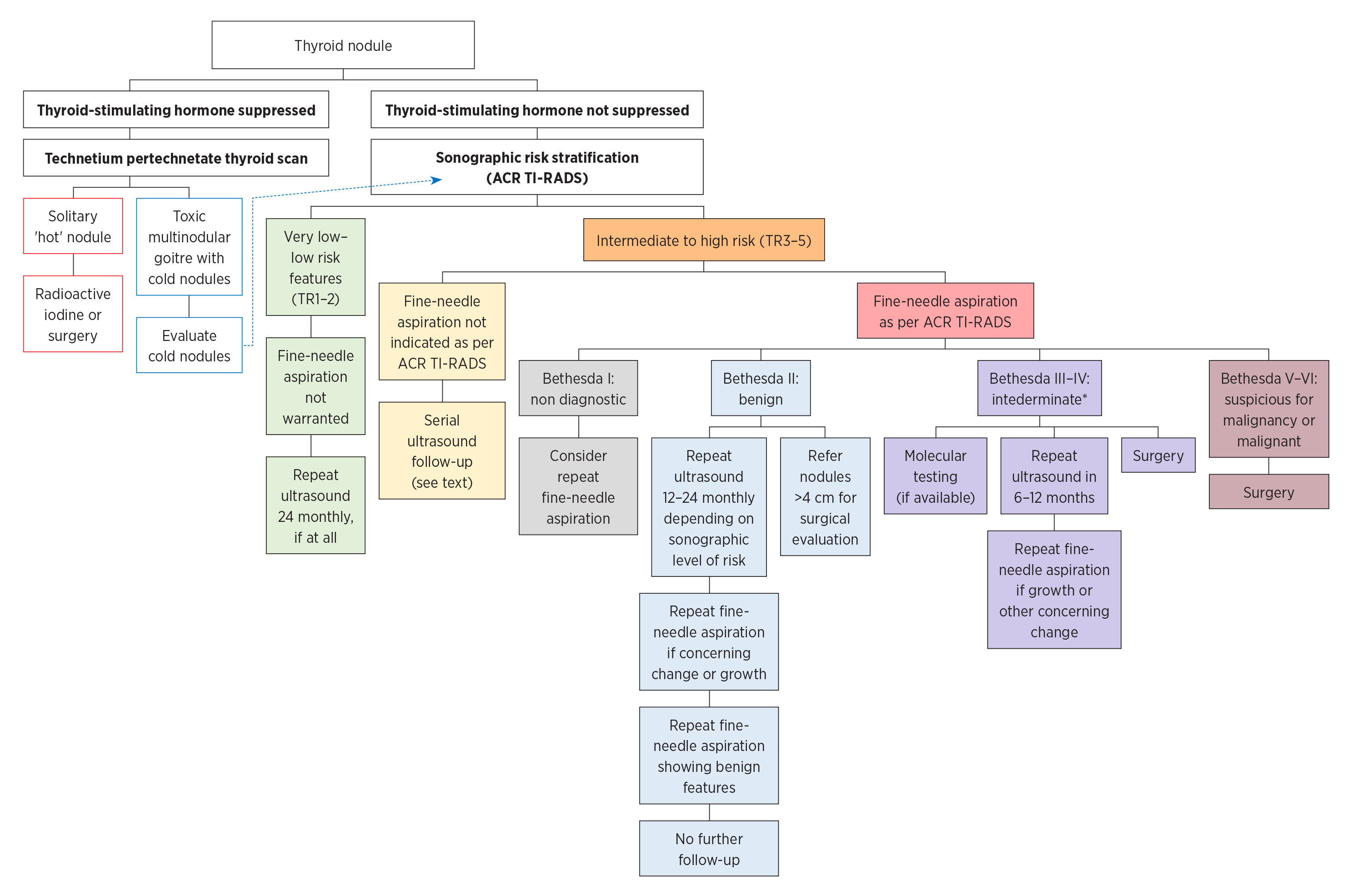
ACR TI-RADS = American College of Radiology Thyroid Imaging, Reporting and Data System
TR = TI-RADS level of risk
* There is no clear approach. Shared decision making may take into account the molecular testing results (if available) and patient preference.
The presence of risk factors and clinical features of thyroid cancer (Table 1) should be sought. However, the history is rarely helpful in differentiating benign and malignant nodules, except if there is a history of irradiation of the head and neck in childhood. This is the greatest risk factor for thyroid malignancy as the risk of carcinoma in nodules in this group is 35–40%.12
Table 1 - Risk of malignancy and criteria for fine-needle aspiration of thyroid nodules19
| ACR TI-RADS classification | Risk of malignancy | Criteria for follow-up* | Criteria for fine-needle aspiration |
| TR1 – benign | 2% | Not required | Not required |
| TR2 – not suspicious | 2% | Not required | Not required |
| TR3 – mildly suspicious | 5% | ≥1.5 cm | ≥2.5 cm |
| TR4 – moderately suspicious | 5–20% | ≥1 cm | ≥1.5 cm |
| TR5 – highly suspicious | ≥20% | ≥0.5 cm | ≥1 cm |
ACR TI-RADS = American College of Radiology Thyroid Imaging, Reporting and Data System
TR = TI-RADS level of risk
* Refer to the section on ‘Monitoring’ for further information.
Measuring thyroid-stimulating hormone is helpful. A suppressed concentration suggests that a nodule is likely to be hyperfunctioning. This should be confirmed with a technetium (Tc-99m) pertechnetate uptake scan (Fig.).13 These scans are not indicated for assessing a nodule in patients who are euthyroid or hypothyroid. Hyperfunctioning nodules are almost never malignant.7
Testing for thyroid peroxidase antibodies, thyroglobulin antibodies or serum thyroglobulin is not indicated as these tests do not aid the diagnosis.13 Thyroid-stimulating hormone receptor antibodies or thyroid-stimulating immunoglobulins can be measured to assess for the presence of Graves’ disease in patients with hyperthyroidism.14
Measurement of serum calcitonin to check for medullary thyroid cancer is not recommended in routine clinical practice given the high risk of false-positive results. This reflects the low prevalence of medullary thyroid cancer in thyroid nodules (0.1–1.4%).2,15 Measurement can be considered in patients who have a family history of medullary thyroid cancer or multiple endocrine neoplasia type 2. However, it should be noted that hypercalcitoninaemia is not pathognomonic of medullary thyroid cancer and there are numerous other causes including certain drugs and chronic autoimmune thyroiditis.2,15,16
Dedicated thyroid ultrasound (including evaluation of anterior cervical lymph nodes) is indicated to evaluate palpable thyroid nodules or those found incidentally on imaging performed for other indications. Thyroid ultrasound is not warranted to screen for nodules in individuals who have hypothyroidism or hyperthyroidism in the absence of risk factors or clinical features of thyroid cancer (Box).10
No single sonographic feature can reliably differentiate benign from malignant neoplasms. Furthermore, there is variability between the recognition and accurate reporting of these features.17 This has led to the development of standardised thyroid nodule risk-stratification systems such as the American College of Radiology Thyroid Imaging, Reporting and Data System (ACR TI-RADS). This system is superior to other major risk-stratification systems for evaluating thyroid nodules, because it reduces the number of unnecessary biopsies and has a high negative predictive value.18
The ACR TI-RADS assigns points based on five key aspects of the thyroid nodule. The total number of points categorises the nodule into five levels of increasing risk (TR1–5). Features that are suggestive of thyroid cancer (e.g. more than 90% of the nodule has a solid composition, hypoechogenicity, taller-than-wide shape on transverse view, irregular margins, microcalcifications) result in the nodule being assigned more points. In contrast, nodules with benign features (e.g. purely cystic and spongiform nodules) score fewer points. The size of the nodule in conjunction with the risk score guides the recommendation for cytological evaluation (Table 1).
There are other thyroid nodule risk-stratification systems, such as the American Thyroid Association (ATA) guideline. This also categorises nodules into five levels of risk, but smaller and lower risk nodules are recommended for biopsy, in contrast to ACR TI-RADS.2 All the major risk-stratification systems generally do not recommend biopsy for nodules that are below 1 cm in size in the absence of high-risk features, such as suspicious cervical lymphadenopathy.2,18
Nodules that do not meet the criteria for biopsy may require re-imaging at periodic intervals to check for new suspicious sonographic changes or growth (≥20% increase in at least two nodule diameters of ≥2 mm, or ≥50% increase in nodule volume).17 Nodules that exhibit these changes should be referred for cytological evaluation.
There is little consensus about the best interval for repeat ultrasonography or duration of follow-up. The ACR TI-RADS recommends that nodules above a certain size threshold (Table 1) be imaged again at certain intervals, assuming that there are no changes between serial ultrasound scans. TR3 nodules are recommended for repeat ultrasound at one, three and five years, TR4 nodules at one, two, three and five years. Annual scans of TR5 nodules are recommended for five years. The ACR TI-RADS does not recommend re-imaging of TR1–2 nodules or smaller TR3–5 nodules (TR3 nodule <1.5 cm, TR4 nodule <1 cm, TR5 nodule <0.5 cm) (Table 1).19 Clinicians may consider re-imaging of TR1–2 nodules at 24-month intervals and the smaller TR3–5 nodules at 12–24-month intervals.2,17 Routine follow-up of purely cystic or spongiform nodules of 1 cm or less is not recommended.2,4
The recommended duration of long-term follow-up of nodules that remain stable and continue to display low-risk features on serial sonographic assessment is five years, as these nodules have a very low risk of harbouring an undiagnosed malignancy.19,20 Nodules that have not met the criteria for biopsy after five years of ultrasound surveillance, but still have suspicious features, such as TR3–5 nodules, may be considered for further evaluation or ongoing surveillance.19 This should be judged on an individual basis, taking into consideration the characteristics of the nodule, patient’s age and comorbid conditions.
Cytological evaluation is warranted for suspicious nodules (Table 2). Thyroid nodules with increased uptake on a Tc-99m pertechnetate scan (so-called ‘hot’ nodules) rarely harbour a malignancy and further evaluation with a biopsy is generally not required.7 However, the presence of suspicious sonographic features in these nodules may merit further evaluation and this should be judged on an individual basis. Suspicious cervical lymph nodes should also undergo fine-needle aspiration with a thyroglobulin washout.2
Table 2 - Bethesda System for Reporting Thyroid Cytopathology21
| Bethesda category | Risk of malignancy | Comment |
| I – Non-diagnostic | 5–10% | Insufficient sample of follicular cells or sample has degraded |
| II – Benign | 0–3% | |
| III – Atypia of undetermined significance or follicular lesion of undetermined significance | 10–30% | Categories III and IV reflect the inherent limitations of cytology – being unable to distinguish between benign versus malignant follicular patterned lesions given the inability to analyse the tissue architecture |
| IV – Follicular neoplasm or suspicious of a follicular neoplasm | 25–40% | |
| V – Suspicious of malignancy | 50–75% | Subtle or focal features of malignancy within the sample |
| VI – Malignant | 97–99% |
Samples from thyroid nodules are reported according to the Bethesda System for Reporting Thyroid Cytopathology (Table 2).21 Approximately 15% of samples are non-diagnostic (Bethesda I), requiring clinicians to revisit the radiological characteristics to determine whether a repeat biopsy is warranted, ideally within 1–2 months.13 Diagnostic accuracy can be improved by having an on-site pathologist available to review the adequacy of the fine-needle aspiration sample at the time of biopsy.7
Approximately 70% of samples are reported as having benign cytology (Bethesda II), generally indicating a low risk of malignancy. However, these results should be interpreted in conjunction with ultrasound findings. Suspicious nodules seen on ultrasound warrant follow-up within 12 months.4 It is uncertain whether nodules that are larger than 4 cm with benign cytology are more likely to harbour a malignancy. These patients should be referred to a surgeon for consideration of further evaluation.2,7
Around 10–15% of samples are reported as intermediate (Bethesda III–IV). The options for further evaluation include ultrasound follow-up, repeat fine-needle aspiration, or diagnostic lobectomy.
Molecular testing for genetic alterations that convey a higher risk of malignancy are being increasingly used in the USA to help further risk stratification of nodules with indeterminate cytology.17 However, these tests are not routinely available in Australia and are not subsidised. Several Australian centres are developing this analysis. Thyroid surgeons and endocrinologists can discuss this investigation with interested patients.
Cytology that is classified as suspicious for malignancy or malignant (Bethesda V–VI) is an indication to refer the patient to a surgeon experienced in the management of thyroid cancer.7,13,17
When there is uncertainty regarding further management, consultation with an endocrinologist experienced in the management of thyroid cancer is advised.
The initial management for confirmed thyroid cancer is surgical, with a total (or near-total) thyroidectomy with or without dissection of the anterior cervical lymph nodes. A lobectomy may be offered in certain low-risk cancers or microcarcinoma (diameter <1 cm).2
Surgery is recommended for multinodular goitres that are causing compressive symptoms. Hyperfunctioning thyroid nodules can be treated with surgery or radioactive iodine ablation.2 Hypothyroidism should be appropriately treated.
Thyroxine suppressive therapy to retard nodule growth is not recommended. It has not been shown to be effective and is associated with an increased risk of cardiac arrythmia and osteoporosis.2
During pregnancy, thyroid nodules generally tend to enlarge with gestational age. This does not necessarily mean that a nodule is malignant. Nodules detected during pregnancy should undergo the standard evaluation processes, except for a Tc-99m pertechnetate thyroid uptake scan as this is contraindicated in pregnancy. Women who are diagnosed with differentiated thyroid cancer during pregnancy are often able to have their surgery safely postponed until after delivery.2
Thyroid nodules are a common clinical finding, often presenting incidentally during radiology performed for the investigation of non-thyroidal illness. While most thyroid nodules are benign, all patients should undergo a stepwise evaluation. This includes with sonographic characterisation and, when indicated, cytological evaluation to determine the likelihood of underlying malignancy. Individuals diagnosed with thyroid cancer should be referred for surgical management.
Conflicts of interest: none declared
This article is peer-reviewed.
Australian Prescriber welcomes Feedback.
Senior staff specialist, Southern Adelaide Diabetes and Endocrine Services, Southern Adelaide Local Health Network

