Article
Management of acute bleeding in the upper gastrointestinal tract
- Daniel L. Worthley, Robert J. Fraser
- Aust Prescr 2005;28:62-6
- 1 June 2005
- DOI: 10.18773/austprescr.2005.051
Acute upper gastrointestinal haemorrhage is common. Patients require simultaneous resuscitation and clinical assessment followed by referral for endoscopy. There have been significant developments in terms of the acute endoscopic and medical treatment of upper gastrointestinal haemorrhage, as well as the development of prognostic tools to help guide management. Preventing recurrent haemorrhage is also important. This requires an understanding of both the aetiology and risk factors for recurrence, as well as the medical and endoscopic treatments available to reduce these risks.
Acute upper gastrointestinal haemorrhage (bleeding proximal to the duodenojejunal flexure) is a common medical emergency (170 per 100 000 adults annually). Although its incidence may be declining, the mortality rate of upper gastrointestinal haemorrhage remains high, approximately 6-8%.1 Depending on the site and rate of bleeding, a patient may present with melaena (black, tarry stool), haematemesis (vomiting 'coffee-grounds' or fresh blood), haematochezia (red blood per rectum) or syncope. Melaena may also result from bleeding into the more distal small intestine or proximal colon.
The majority of patients with upper gastrointestinal haemorrhage require hospital management. General practitioners have an important role in assessing and resuscitating patients and then managing them following discharge to reduce the risk of recurrent bleeding.
Initial clinical assessment is directed towards the haemodynamic stability of the patient and the requirement for immediate resuscitation.
The presenting symptom, past medical history and current medications are important for establishing the aetiology (see Box and Table 1) and severity of haemorrhage. A history of recent dyspepsia, or use of aspirin or another non-steroidal anti-inflammatory drug (NSAID) may suggest a bleeding ulcer. The presence of chronic liver disease raises the possibility of variceal haemorrhage.
Haematemesis that follows prolonged vomiting or retching may be the result of a Mallory-Weiss tear. A history of syncope may reflect haemodynamically significant bleeding. Vomiting frank blood suggests severe haemorrhage from an arterial or variceal source. In contrast, 'coffee-grounds' emesis is unlikely to reflect active bleeding.
Approximately 50-100 mL of blood is needed to produce melaena. Haematochezia may occur with brisk upper gastrointestinal haemorrhage and is usually accompanied by haemodynamic compromise.
It is critical to assess the patient's haemodynamic status by measuring heart rate, blood pressure and postural changes. In haemodynamically compromised patients a fall in blood pressure may follow only a minor change in posture, for example from lying flat to sitting at a 450 incline. Variceal haemorrhage is more likely if stigmata of chronic liver disease are present, particularly if there is evidence of portal hypertension, for example ascites and splenomegaly. An ulcer may cause epigastric tenderness. Digital rectal examination is important to confirm the presence of true melaena.
Haemoglobin needs to be measured in all patients but may initially underestimate true blood loss, due to delayed haemodilution of the vascular space. Blood should be sent urgently to transfusion services for cross-matching. Other important tests include platelet count, urea:creatinine ratio, coagulation indices and liver function tests including albumin. Patients with end stage liver disease may have normal liver enzymes, yet have impaired synthetic liver function as evidenced by low albumin, or reduced clotting factors.
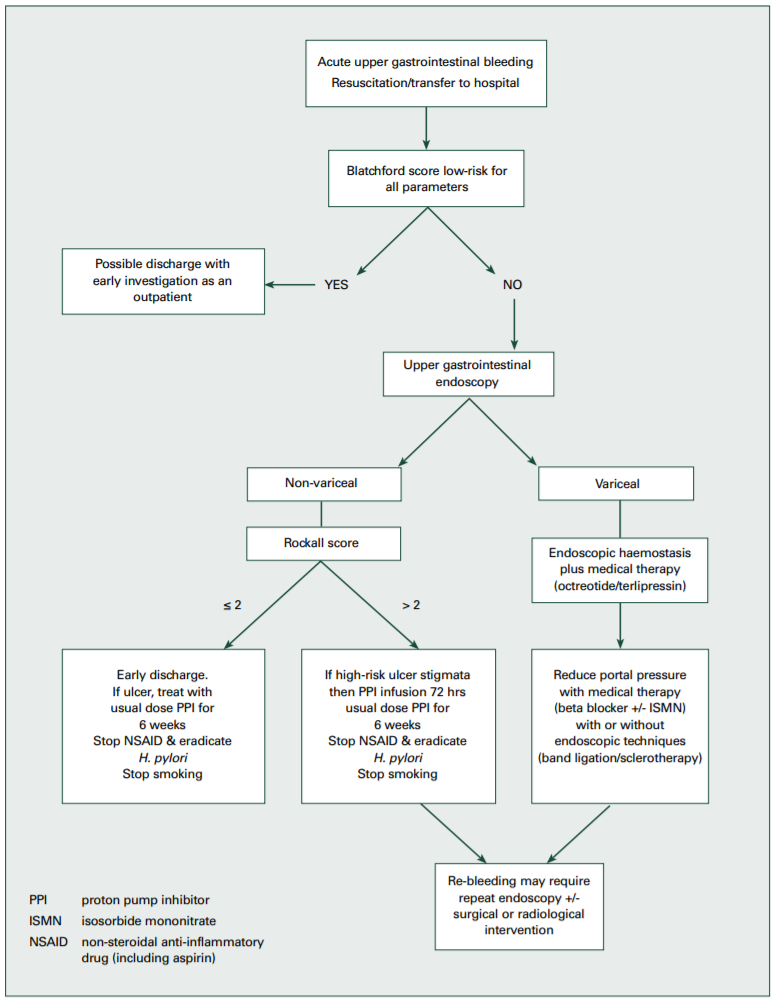
The Blatchford score predicts the need for therapy and thus admission. Patients are unlikely to need treatment and therefore may not require admission if they satisfy the following criteria:
This 'fast-track' triage could be used in an emergency department to avoid unnecessary admissions.2 Likewise in regional areas, such a scoring system could help the general practitioner decide if a patient requires immediate transfer to a tertiary referral centre, or whether it is reasonable to discharge the patient with a view to arranging an early outpatient endoscopy at the closest facility. The safety of using the management algorithm in this way is yet to be formally evaluated, and thus patients should continue to be managed on a case by case basis.
The Rockall score is frequently used for risk categorisation (Table 2). The score is the sum of each component, calculated before and after endoscopy. This predicts rates of re-bleeding and mortality and can be used in management algorithms, for example whether to admit a patient to an intensive care unit. Post-endoscopy risk scores of 2 or less are associated with a 4% risk of re-bleed and 0.1% mortality. In one study about 30% of patients had post-endoscopy risk scores of 2 or less and thus significant health savings could be achieved by early endoscopy and discharge.3
Until cross-matched blood is available, resuscitation proceeds with crystalloid or colloid solutions aiming for a systolic blood pressure of greater than 100 mmHg. Thiamine replacement should be considered when there is a history of alcohol abuse.
The target haemoglobin concentration is contentious. Some advocate 70-80 g/L for otherwise healthy individuals, without active bleeding, who are haemodynamically stable.4In patients older than 65 or those with cardiovascular disease a target concentration of 90-100 g/L may be more appropriate.
After resuscitation an endoscopy is arranged. Some patients with profuse haemorrhage require emergency endoscopy, however the majority can be scheduled on the next routine list. The endoscopy should, however, take place within 24 hours of presentation, both to guide management and to facilitate the early discharge of patients with a low risk of recurrent bleeding.
When high-risk lesions are seen (ulcers with active spurting vessel or non-bleeding visible vessel) endoscopic therapy significantly reduces re-bleeding rates and mortality.1 A dual-modality endoscopic approach is currently recommended, with a combination of (1:10 000) adrenaline injection and thermal coagulation.
Band ligation and sclerotherapy are the two main endoscopic techniques for treating acute oesophageal varices.5 These procedures are less successful in gastric varices, although injection with tissue adhesive may be effective.
In gastrointestinal haemorrhage there is enhanced mucosal fibrinolytic activity, impairing haemostasis.6 Suppressing acid secretion blunts this escalation in fibrinolysis. In this setting high-dose proton pump inhibitor therapy reduces the risk of recurrent bleeding.7
Proton pump inhibitor therapy can be administered parenterally (either intermittently or by infusion) or orally. When high-risk features are present at endoscopy it may be advisable to administer high dose intravenous proton pump inhibitor therapy, that is omeprazole 80 mg (or equivalent) bolus followed by an infusion rate of 8 mg/hour for 72 hours. Where the cost of intravenous proton pump therapy is prohibitive and especially when there are no high-risk ulcer features, an oral proton pump inhibitor may be satisfactory.7
Medical therapy reduces variceal bleeding by lowering portal venous pressure. The available drugs include vasopressin and its synthetic analogue terlipressin, as well as somatostatin and its synthetic analogues octreotide and vapreotide. The relative merits of these drugs are unclear. The addition of an octreotide infusion to endoscopic therapy improves bleeding control and reduces transfusion requirements,5 therefore a combination of endoscopic and medical treatment is probably the best approach. However, only terlipressin has been shown to reduce mortality rates following variceal bleeding,8 but it is currently only available in Australia under the Special Access Scheme.*
It is important to remember that variceal haemorrhage may precipitate hepatic encephalopathy. Re-bleeding from varices or ulcers may require repeat endoscopy. Sometimes endoscopic therapy is unsuccessful and surgery is needed. See Fig. 1.
Prevention of recurrent bleeding in ulcer disease should be directed towards the underlying cause. All patients should be asked about aspirin and other NSAID use and be tested for Helicobacter pylori. Patients who smoke should be advised to stop.
NSAIDs should be discontinued where possible. The ulcer may then be healed with an H2-receptor antagonist or a proton pump inhibitor over a period of six weeks.9 Current clinical practice favours proton pump inhibitor therapy over H2-receptor antagonist for ulcer healing. No further endoscopy is required for duodenal ulcers, but repeat endoscopy at eight weeks is advisable for gastric ulcers to ensure healing and exclude malignancy.
In patients requiring ongoing NSAID therapy, a concomitant proton pump inhibitor achieves a greater rate of ulcer healing than H2-receptor antagonists.10 An alternative approach is to substitute paracetamol or a COX-2 selective drug for the conventional NSAID. In terms of the rate of recurrent bleeding, this strategy is comparable to taking a conventional NSAID with a proton pump inhibitor.11 The rate of recurrent haemorrhage in this group, however, is still relatively high. It is important to remember that the gastrointestinal advantages of COX-2 selective inhibitors are negated by concomitant aspirin therapy, and that there has been recent concern about the cardiovascular safety of this class of drug. A proton pump inhibitor reduces the risk of recurrent bleeding when long-term aspirin therapy is required. The timing of the resumption of a medication which may have contributed to the gastrointestinal haemorrhage should balance the likelihood of re-bleeding, the indication for the drug and whether safer alternatives are available.
All patients with ulcer disease should be tested for H. pylori 12 and the bacteria eradicated if found. Successful eradication, usually a seven day regimen of triple therapy, significantly reduces the risk of ulcer recurrence.13 Once H. pylori eradication is confirmed and the ulcer has been healed by six weeks of treatment with an H2-receptor antagonist or proton pump inhibitor, no further therapy is required.
A number of patients have ulcers without a clear aetiology. These patients should have their ulcers healed with either an H2-receptor antagonist or a proton pump inhibitor for 6-8 weeks.9 However, they may require long-term acid suppression.
Variceal bleeding recurs in approximately two-thirds of patients.5 Both endoscopic and medical strategies are used in an attempt to reduce recurrent oesophageal variceal bleeding. Regular endoscopic treatment, usually 3-4 sessions (initially weekly, then every 2-3 weeks), with either sclerotherapy or banding can obliterate oesophageal varices. Band ligation is preferred because of greater efficacy and a lower incidence of oesophageal strictures.5 Alternatively, reducing portal pressure with a non-selective beta blocker (propranolol, nadolol (not approved in Australia)) with or without a long-acting nitrate has proven effective. The combination of nadolol and isosorbide mononitrate therapy was superior to band ligation alone in preventing recurrent variceal bleeding.14 It is possible, however, that combination endoscopic and medical therapy (in this study the medical treatment was nadolol and sucralfate) may be more effective than either alone.15 Some patients require specialist techniques such as porto-systemic shunting by surgery or by a transjugular intrahepatic porto-systemic shunt. Other patients may not be able to have optimal medical treatment because of contraindications or adverse effects. In the case of alcoholic liver disease, failure to stop drinking increases the risk for recurrent haemorrhage, so abstention from alcohol is critical.
Management of acute upper gastrointestinal haemorrhage begins with clinical assessment and resuscitation. Endoscopy is required for diagnosis and initial therapy. A combination of medical and endoscopic strategies are used to reduce the risk of recurrent bleeding.
* www.tga.gov.au/docs/html/sasinfo.htm [cited 2005 May 10]
Associate Professor Fraser has received unrestricted grants from AstraZeneca, Pfizer, Lederle, and Altana, and acts as a consultant to Pfizer. Dr Worthley has received travel grants from AstraZeneca.
The following statements are either true or false.
Click anywhere on the panel for the answers.
1. Acute treatment with high doses of proton pump inhibitors reduces the risk of further bleeding after an upper gastrointestinal haemorrhage.
2. A patient needs to lose at least 500 mL of blood into the gut before they develop melaena.
Answers to self-test questions
1. True
2. False
Registrar
Associate Professor and Director of Gastroenterology, Repatriation General Hospital, Daw Park, South Australia
