Article
Management of Bell’s palsy
- Dhruvashree Somasundara, Frank Sullivan
- Aust Prescr 2017;40:94-7
- 1 June 2017
- DOI: 10.18773/austprescr.2017.030
Bell’s palsy is facial nerve paralysis of unknown cause. Left untreated, 70–75% of patients make a full recovery.
Early treatment with prednisolone increases the chance of complete recovery of facial function to 82%. Eleven people need to be treated for one extra complete recovery at six months.
There may be benefit in adding an antiviral drug to prednisolone in some cases. Additional research is needed on this treatment.
The palsy may leave the surface of the eye exposed. Early eye protection with lubrication and a patch is crucial to prevent long-term complications.
Bell’s palsy, also called idiopathic facial paralysis, is defined as an acute-onset, isolated, unilateral, lower motor neurone facial weakness. The reported annual incidence varies in different parts of the world with estimates varying between 11 and 40 per 100 000 people.1 It is more common in people with diabetes.2
The underlying pathophysiology observed in post mortem cases of Bell’s palsy is vascular distension, inflammation and oedema with ischaemia of the facial nerve. The aetiology remains unclear. Various causes have been proposed including viral, inflammatory, autoimmune and vascular. However, reactivation of herpes simplex virus or herpes zoster virus from the geniculate ganglion is suspected to be the most likely cause.3,4 Despite advances in neuroimaging, the diagnosis of Bell’s palsy is mainly clinical.5
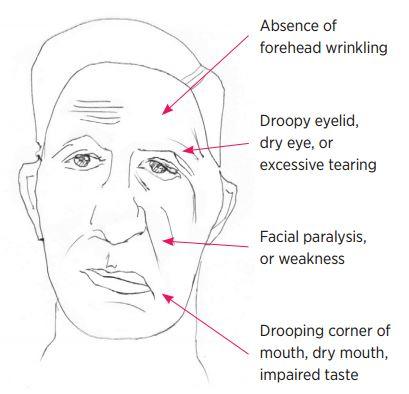
Symptoms and signs of Bell’s palsy (see Fig. and Box) can vary from mild to severe. There are several conditions to consider in the differential diagnosis:
In addition to ocular problems, complications of Bell’s palsy include:
Box
The severity of symptoms of Bell’s palsy varies from mild weakness to severe paralysis, but the prognosis is generally good. The Copenhagen Facial Nerve Study found that around 71% of patients recover normal function without treatment. Around 13% are left with slight weakness and around 4% with severe weakness resulting in major facial dysfunction. Contracture of the facial muscles on the affected side was found in 17% and associated movements were found in 16%.6 Scoring systems such as the House–Brackmann scale used in randomised controlled trials and systematic reviews may be helpful to monitor progress.7
Although the study was underpowered to detect significant differences in recovery between patients with different degrees of severity, the recovery rate in one randomised controlled trial was significantly higher for those with moderate severity at onset compared to those with severe Bell’s palsy. Recovery was 90% with those moderately affected and 78% in those severely affected.8
The frequency of review depends on the individual patient and the severity of their symptoms. If there is no improvement after a month the patient should be referred. A referral is also indicated if there is only partial recovery after 6–9 months.
The palsy recurs in 7% of patients, with equal incidence of ipsilateral and contralateral recurrence. There are insufficient data on whether treatment affects the rate of recurrence.
The treatment of Bell’s palsy aims to speed recovery and reduce long-term complications. An inability to close the eye on the affected side increases the risk of corneal complications. Eye protection is crucial so an eye patch and lubricants are used to prevent drying of the cornea. Eye drops, such as hypromellose drops, should be applied for lubrication during the day and ointment at night. In severe cases, the eye may have to be taped or partially sutured shut.
The treatments considered for Bell’s palsy include oral corticosteroids (prednisolone) and antiviral drugs. Although the aetiology of Bell’s palsy is uncertain, it is known that inflammation and oedema of the facial nerve are responsible for the symptoms. Corticosteroids have therefore been used for their anti-inflammatory effect.
The maximum benefit is seen when steroids are commenced within 72 hours of the onset of symptoms. There is no optimum regimen, but in adults 50–60 mg prednisolone daily for 10 days has been commonly used.6,7 Prednisolone has been used at a dose of 1 mg/kg/day up to a maximum of 80 mg in some studies. Doses of more than 120 mg/day have been used safely in patients with diabetes.9
In a randomised controlled trial the recovery rate at nine months with prednisolone was 94%. It was 81.6% in patients who did not receive prednisolone.7
A systematic review of trials that used prednisolone showed that at six months 17% of patients had incomplete recovery compared with 28% of patients who received no treatment. There was also a significant reduction in motor synkinesis in those who received prednisolone. There was no significant reduction in cosmetically disabling sequelae.10
The antiviral drugs used in trials were aciclovir (400 mg five times daily for five days) or valaciclovir (1000 mg/day for five days).11 There is currently no evidence to support the use of either antiviral drug on its own,12,13 and there is uncertainty regarding the benefit of adding them to corticosteroids.
A randomised controlled trial found that at nine months of diagnosis, facial function had recovered in 94.4% of patients who took prednisolone alone, 85.4% of those who took aciclovir alone and 92.7% of those who received both. There were no serious adverse effects in any group. The study concluded that early treatment with prednisolone alone increases the likelihood of complete recovery and there was no additional benefit of treatment with aciclovir alone or combining with prednisolone.7 However, a systematic review also found that treatment with prednisolone reduced the chances of incomplete recovery but using an antiviral drug had an additional benefit.14
There have been several studies looking at the benefit of antiviral drugs with or without prednisolone. A randomised prospective study found that a combination of an antiviral and a steroid was more effective in treating severe to complete Bell’s palsy than steroid alone.15 A guideline development group found that there was low-quality evidence of benefit from adding antivirals. Patients who are offered them in addition to corticosteroids should be counselled that the increase in recovery is less than 7%.16
A Cochrane review in 2015 found that antivirals combined with corticosteroids improved rates of incomplete recovery compared with corticosteroids alone, but this was not significant and the evidence was low quality. There was moderate-quality evidence that the combination reduced long-term sequelae such as excessive tear production and synkinesis. The outcome for patients who received corticosteroids alone was significantly better than for those who received antivirals alone. Antiviral drugs alone had no benefit over placebo. None of the treatments had significant differences in adverse effects, but the evidence was again of low quality.12
The optimum management of children with Bell’s palsy is also unknown. A major trial (BellPIC) in Australia is addressing this question.17
Treatment courses are short, but can cause adverse effects.
Prednisolone should be used with caution in immunosuppression and sepsis. It may lead to:
Antiviral drugs may cause:
Physical therapies including tailored facial exercises, acupuncture to affected muscles, massage, thermotherapy and electrical stimulation have been used to hasten recovery. However, there is no evidence for any significant benefit. A Cochrane review concluded from poor-quality evidence that tailored facial exercises can help improve facial function, mainly for moderate paralysis and chronic cases. Early facial exercise may reduce recovery time, long-term paralysis and number of chronic cases.18
Surgical treatment to free the facial nerve has been considered. However the evidence for this procedure is of very low quality.19-21
The symptoms of Bell’s palsy vary from mild to severe. The aetiology is still unclear, but it is known that the symptoms are caused by swelling and inflammation of the facial nerve. Eye protection remains crucial in preventing long-term eye complications.
Drug treatment is controversial, given that over 70% of patients will eventually recover normal facial function without treatment. Early treatment with prednisolone can hasten recovery and reduce long-term sequelae. Although the quality of evidence is low to moderate, there may be some benefit in adding antiviral drugs to prednisolone.12 It is, however, important to discuss the harms and benefits with patients, given the potential adverse effects of prednisolone and antiviral drugs.
Conflict of interest: none declared

General practitioner, NHS Tayside Dundee, Scotland
Gordon F Cheesbrough research chair and Director of UTOPIAN FMTU, North York General Hospital, Toronto, Ontario, Canada
Professor, Department of Family and Community Medicine and Dalla Lana School of Public Health, University of Toronto, Ontario, Canada
Adjunct scientist, Institute for Clinical Evaluative Sciences, Toronto, Ontario, Canada
