Article
Managing medicines in alcohol-associated liver disease: a practical review
- Amy L Johnson, Kelly L Hayward
- Aust Prescr 2021;44:96-106
- 1 June 2021
- DOI: 10.18773/austprescr.2021.015
People with alcohol-associated liver disease often take medicines to manage complications of liver disease and comorbidities. However, patients may be at increased risk of drug-related harm.
Assessing the severity of liver disease is fundamental to management, as disease staging (steatosis, early fibrosis, cirrhosis) affects medication safety and guides treatment.
While clinically significant pharmacokinetic and pharmacodynamic changes predominantly occur in cirrhosis, people with early alcohol-associated liver disease may still experience adverse events with potentially inappropriate medicines such as proton pump inhibitors, opioids and benzodiazepines.
Regular medication review is essential to ensure ongoing appropriateness and safety.
Alcoholic hepatitis and cirrhosis require specialist gastroenterology or hepatology management. However, general practitioners will remain the cornerstone of day-to-day medication management.
Alcohol-associated liver disease is one of the major causes of chronic liver disease in Australia. National guidelines recommend healthy adults consume no more than 10 standard drinks per week and a maximum of four standard drinks on any one day.1 However, the Australian Bureau of Statistics 2017–18 National Health Survey found that 16.1% of adults drank an average of at least two standard drinks per day, and 42.1% consumed more than four standard drinks on one occasion in the past year.2
Alcohol use disorder is a severe chronic drinking problem that is characterised by impaired ability to stop or control alcohol use despite adverse social, occupational or health consequences.3 The risk of developing alcohol-associated liver disease increases with the amount of alcohol consumed.4 Between 10 and 35% of excessive drinkers will develop advanced disease.4 People with alcohol-associated liver disease are also at greater risk of cirrhosis-related complications (‘decompensation’) and liver-related death compared to other chronic liver diseases.5 It is important to note that there are no safe limits of alcohol use in patients with alcohol-associated liver disease.
Optimising medicines to manage complications of liver disease and comorbidities can be difficult due to:
Primary care clinicians are ideally placed to improve medication safety by reviewing and monitoring a patient’s medicines and reducing use of potentially inappropriate medicines.
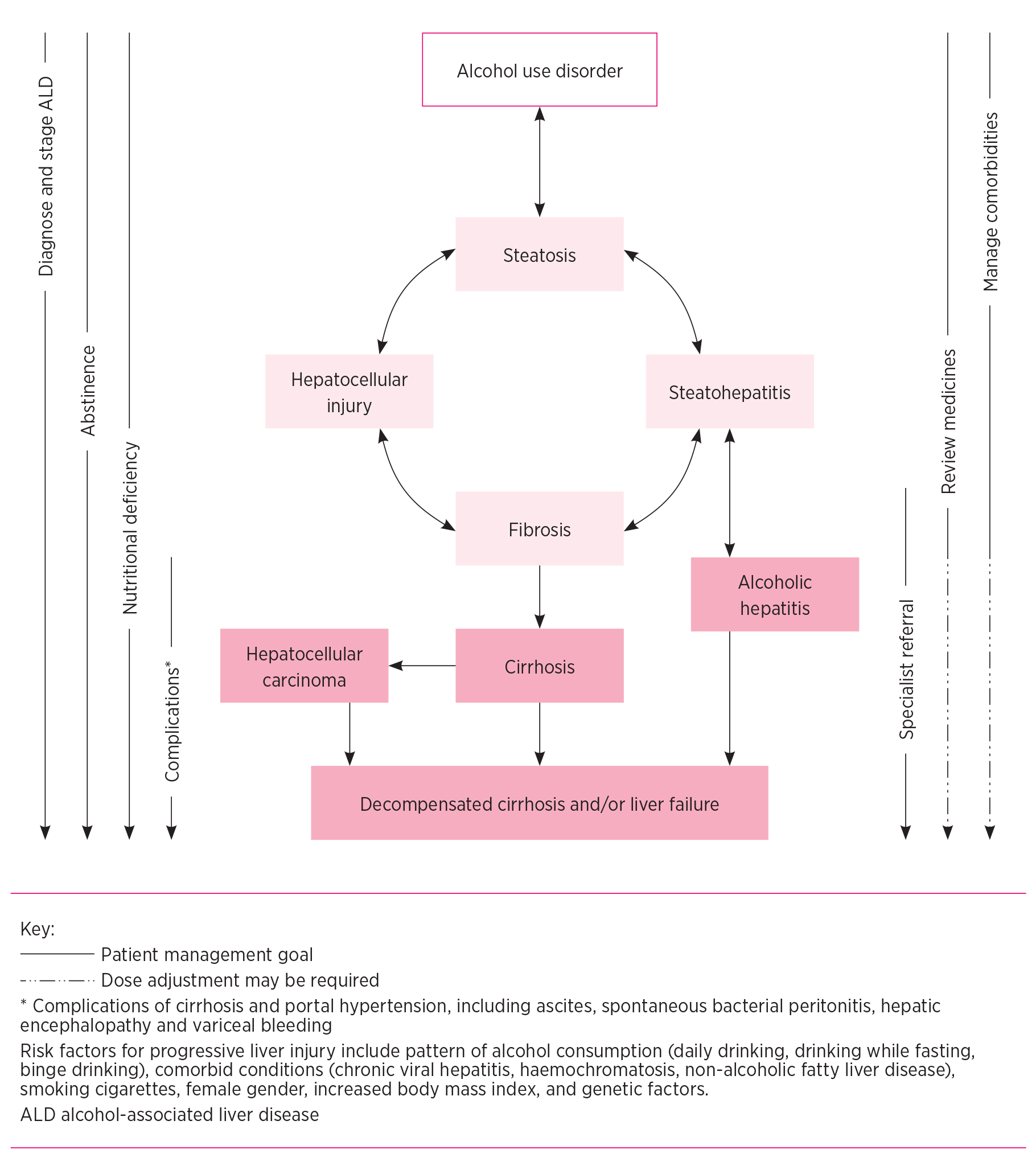
The role of medicines in alcohol-associated liver disease and the goals of treatment evolve with progression of disease. Optimisation of medicine use and minimisation of medicine-related harm therefore relies on appropriate staging.
The pathogenesis of alcohol-associated liver disease is complex. The disease spectrum ranges from simple hepatic steatosis to more advanced forms, including alcoholic hepatitis, alcoholic cirrhosis, and acute-on-chronic liver failure (see Fig.).6 Investigations to assist with staging include medical imaging (ultrasound, magnetic resonance imaging, computed tomography), transient elastography (FibroScan), and tests such as Fibrosis-4, aspartate aminotransferase:alanine aminotransferase ratio, and aspartate aminotransferase platelet ratio index.7,8
Unlike renal disease, in which there are relatively reliable measures of glomerular filtration, there is no simple measure of hepatic function to guide drug dosing in liver disease. However, patterns and markers in common blood tests can suggest acute hepatic inflammation or impaired synthetic function and may assist decision making regarding the safety of medicines (Table 1).9-17
Table 1 - Abnormal blood tests and medication considerations in people with alcohol-associated liver disease9-17
|
Parameter |
Test result |
Comment |
|
Aspartate aminotransferase (AST)* |
Usually <8 times upper limit of normal.† AST is often higher than ALT with a ratio >1:1. Typically between 50–400 IU/mL in alcoholic hepatitis with AST often higher than ALT (ratio >2:1). May be ‘normal’ in cirrhosis. |
Review drugs that may contribute to liver function test derangement and hyperbilirubinaemia: • antibiotics • antiepileptics • herbal and dietary supplements • paracetamol • statins. These tests do not reflect hepatic capacity to metabolise or clear medications, except where acute liver failure or cirrhosis is suspected. |
|
Alanine aminotransferase (ALT)* |
Usually <5 times upper limit of normal.† Elevated in alcoholic hepatitis but usually <400 IU/mL with ALT often lower than AST as above. May be ‘normal’ in cirrhosis. |
|
|
Alkaline phosphatase |
Usually <2–3 times upper limit of normal. |
|
|
Gamma-glutamyl transferase |
Often elevated in heavy drinkers, but non-specific. Other causes of elevation include: • biliary obstruction/disease • medications (e.g. phenytoin, barbiturates). |
|
|
Bilirubin |
Often elevated (>50 micromol/L) in alcoholic hepatitis and cirrhosis due to impaired liver synthetic function. Higher bilirubin concentrations indicate more severe alcoholic hepatitis and onset of jaundice usually occurs within the preceding 8 weeks.‡ Elevation can signify decompensation in cirrhosis. |
|
|
Haemoglobin |
May be low in all stages of alcohol-associated liver disease due to multiple factors. |
Check iron studies and replace if deficient. Anticoagulant and antiplatelet therapies for comorbidities should be continued (if indicated) unless bleeding is suspected. |
|
Lymphocytes and neutrophils |
May be reduced in portal hypertension and cirrhosis due to hypersplenism. White cell count is elevated in alcoholic hepatitis, but usually <20 x 109/L (largely neutrophils). |
Use drugs that can impair immunity with caution and monitor regularly: • corticosteroids • azathioprine. |
|
International normalised ratio/prothrombin time |
Often elevated in alcoholic hepatitis and cirrhosis due to impaired synthetic function and reduced hepatic production of coagulation factors. |
INR is a good measure of liver synthetic function but not bleeding risk. Decompensated cirrhosis is a prothrombotic state. Monitoring parameters for anticoagulant therapies (warfarin, heparin, low-molecular-weight heparin) may be less reliable. Vitamin K supplementation is only helpful in deficiency. |
|
Albumin |
May be reduced in alcoholic hepatitis and cirrhosis due to impaired synthetic function and reduced hepatic production of proteins. |
Distribution of highly protein-bound drugs may be altered: • valproate, phenytoin • warfarin • diazepam. |
|
Platelets |
Often low in cirrhosis due to bone marrow suppression and splenic sequestration associated with portal hypertension. |
Prophylactic use of heparin and low-molecular-weight heparin is usually avoided, particularly when platelet count <50 x 109/L. Use of aspirin in coronary artery disease appears safe. |
|
Sodium |
May be low in alcoholic hepatitis and cirrhosis due to altered renal haemodynamics, renin–angiotensin–aldosterone system dysregulation and fluid accumulation. |
Avoid or carefully monitor drugs that may worsen hyponatraemia or renal function: • ACE inhibitors, sartans • diuretics. |
|
Creatinine |
May be elevated in decompensation, hepatorenal syndrome and severe alcoholic hepatitis. Baseline creatinine may be low in cirrhosis due to low muscle mass. |
Have a low index of suspicion for acute renal impairment in people with cirrhosis due to low baseline creatinine. Use medicines that may affect renal function with caution and monitor required therapies regularly (e.g. diuretics). Nephrotoxic drugs are often withheld in severe alcoholic hepatitis to prevent or manage acute kidney injury and hepatorenal syndrome, which negatively impact survival. |
* Transaminases >400 IU/mL should raise suspicion of other causes of acute liver injury.
† Degree of elevation does not correlate with alcohol-associated liver disease severity.
‡ Clinical history usually includes heavy alcohol use (>40 g/day in women, >60 g/day in men) for at least 6 months with fewer than 60 days of abstinence before onset of jaundice.
Interactions between alcohol and medicines can occur in active drinkers. For example, drugs that accelerate gastric emptying (e.g. metoclopramide, domperidone, erythromycin) and those that inhibit alcohol dehydrogenase activity (e.g. aspirin, ranitidine) may result in higher blood alcohol concentrations.18 This can subsequently increase the risk of pharmacodynamic interactions with sedatives, anticholinergics and antidepressants, and cause symptoms such as increased drowsiness, sedation and decreased motor skills.
Pharmacokinetic interactions with aldehyde dehydrogenase (e.g. disulfiram, metronidazole) can lead to rapid accumulation of ethanol’s bioactive metabolite acetaldehyde and significant adverse effects.18,19 Upregulation of cytochrome P450 2E1 in chronic alcohol use can also affect the metabolism of other drugs (e.g. paracetamol, phenobarbital).18,20 These interactions depend on genetic variability and the presence or absence of alcohol as a competitive substrate.
Despite the potential for increased bioactivation to its toxic metabolite, paracetamol is generally considered safe for most people with alcohol-associated liver disease and is preferred over non-steroidal anti-inflammatory drugs in advanced disease.21 Dose reduction to a maximum 2–3 g of paracetamol daily is recommended for malnourished patients and those with cirrhosis.20,21
Intervention to support abstinence is essential, as cessation of drinking reduces the risk of liver disease progression, and cirrhosis-related complications, and it improves clinical outcomes at all stages.6,22,23 In addition to psychosocial treatments, pharmacotherapy may be prescribed to support abstinence.24 Therapies available on the Pharmaceutical Benefits Scheme in Australia include naltrexone and acamprosate. Disulfiram is also used but is only available on private prescription (Table 2).9,16,19,24-31 These medicines have modest efficacy and most have limited or no published safety data in people with cirrhosis and should only be considered under specialist guidance.6 Other medicines including gabapentin, baclofen and topiramate may be prescribed off label by specialists to assist relapse prevention, but evidence for their effectiveness is limited.6,24
Table 2 - Commonly used medicines in different stages of alcohol-associated liver disease9,16,19,24-31
|
Drugs |
Indication and mechanism of action |
Precautions and contraindications |
Comments |
|
Alcohol abstinence |
|||
|
Acamprosate |
Reduces symptoms of alcohol withdrawal (e.g. anxiety, irritability, insomnia, cravings, neuronal hyperexcitability). Modulates the glutamatergic receptor system. |
Contraindicated: Child-Pugh C cirrhosis, renal impairment (serum creatinine >120 micromol/L or creatinine clearance ≤30 mL/min). Caution: acute alcohol withdrawal, pregnancy. |
Not hepatically metabolised but requires dose adjustment in renal impairment. Alcohol-induced psychomotor impairment will still occur if alcohol is consumed. Commence after the acute phase of alcohol withdrawal has passed (i.e. 1 week after the last drink). |
|
Naltrexone |
Attenuates cravings and reduces pleasurable effects following alcohol consumption. Reversible inhibition of opioid receptors. |
Contraindicated: opioid dependence, severe hepatic impairment, acute hepatitis. Caution: renal impairment, liver enzymes >3 times upper limit of normal. |
Risk of hepatotoxicity in hepatic and renal impairment. Alcohol-induced psychomotor impairment will still occur if alcohol is consumed. Use non-opioid analgesics (e.g. paracetamol) if pain relief is required. |
|
Disulfiram |
Interference with alcohol metabolism. Irreversible inhibition of aldehyde dehydrogenase results in raised blood acetaldehyde concentrations and unpleasant effects if alcohol is consumed. |
Contraindicated: current alcohol intoxication, ischaemic heart disease, severe myocardial disease, severe renal impairment, severe hepatic impairment, acute psychosis, cirrhosis. Caution: cardiovascular disease, diabetes, hypothyroidism, epilepsy, chronic kidney disease, hepatic impairment. |
Not recommended in moderate–severe liver disease due to lack of safety data. Extensive patient and carer education required before starting disulfiram. Adverse effects of a disulfiram–alcohol reaction can be severe, including respiratory depression, seizures, arrhythmia, myocardial infarction and worsening of acute congestive heart failure in patents with pre-existing cardiac conditions. Numerous potential drug–drug interactions. |
|
Alcohol withdrawal syndrome |
|||
|
Benzodiazepines: • diazepam, oxazepam |
Reduce acute alcohol withdrawal symptoms and seizure risk. Modulate neuronal hyperexcitability by stimulating gamma‐aminobutyric acid (GABA) receptors. |
Caution: may precipitate hepatic encephalopathy in patients with cirrhosis or acute liver failure. |
Short-acting benzodiazepines with uncomplicated hepatic metabolism (e.g. oxazepam) are preferred in people with cirrhosis and the elderly. |
|
Alcoholic hepatitis |
|||
|
Corticosteroids: • prednisolone |
Modulate inflammatory response. May improve short-term survival in severe alcoholic hepatitis. |
Contraindicated: untreated infection, gastrointestinal bleeding, renal failure, acute psychosis, pancreatitis (uncontrolled hyperglycaemia). Caution: diabetes, peptic ulcer disease. |
Started in hospital with other supportive care. Short-term use only (up to 4 weeks with optional 3-week taper thereafter). |
|
Nutritional deficiency |
|||
|
Thiamine (B1) |
Chronic thiamine deficiency can lead to nutritional encephalopathy (Wernicke-Korsakoff’s syndrome). |
Thiamine doses contained in over-the-counter oral supplements may be insufficient. |
|
|
Other B vitamins: • pyridoxine (B6), folic acid (B9), cyanocobalamin (B12) |
Prevent complications of deficiency including cognitive dysfunction, peripheral neuropathy, and anaemia. Vitamin B deficiencies are common in alcohol-associated liver disease. |
Caution: folic acid supplementation should be avoided in megaloblastic anaemia until B12 deficiency is corrected. |
Specific deficiencies should be corrected, but evidence is lacking for long-term use. |
|
Vitamin D |
Regulates absorption of essential minerals including calcium, magnesium and phosphate. Vitamin D deficiency is common in patients with cirrhosis. |
Caution: severe renal impairment, hypercalcaemia. |
Evidence for vitamin D supplementation in chronic liver disease is inconclusive. Supplement if deficient or in the presence of other indications (e.g. bone disease). |
|
Zinc |
Prevents complications of deficiency including cognitive dysfunction, hypogonadism, altered immune function and impaired wound healing. Improves gut-mucosal barrier integrity. Zinc deficiency is common and worsens with disease progression. |
Caution: severe renal impairment. |
Evidence supports zinc supplementation to correct deficiency in alcohol-associated liver disease, especially in people with cirrhosis and alcoholic hepatitis. |
|
Complications of advanced liver disease (managed by a specialist) |
|||
|
Non-selective beta blockers: • propranolol, carvedilol |
Prevent bleeding from gastro-oesophageal varices. Induce splanchnic vasoconstriction, thereby decreasing portal blood flow and reducing portal hypertension. |
Caution: bradycardia (45–50 beats/min), severe hypotension, peripheral arterial disease, diabetes, poorly controlled asthma, severe hepatic impairment (carvedilol). |
Usually started at a low dose (propranolol and carvedilol are hepatically metabolised) and titrated to achieve a resting heart rate of 55–60 beats/min while maintaining systolic blood pressure ≥90 mmHg. Selective beta blockers (metoprolol, bisoprolol) are not effective. Carvedilol is not PBS-listed for this indication. |
|
Diuretics: • spironolactone, furosemide (frusemide) |
Treat fluid overload (e.g. ascites, hepatic hydrothorax). Promote excretion of sodium and water. |
Contraindicated: renal failure, severe sodium and fluid depletion. Caution: renal impairment (creatinine clearance <30 mL/min), electrolyte derangement. |
No significant pharmacokinetic changes in liver impairment, but patients may be at increased risk of harmful pharmacodynamic interactions. Regular monitoring of fluid status, renal function and electrolytes is required. Patients are usually on a salt-restricted diet. |
|
Antibiotic prophylaxis: • trimethoprim/ sulfamethoxazole, quinolones |
Prevent recurrence of spontaneous bacterial peritonitis. Reduce pathogenic gut flora. |
Caution: renal impairment (creatinine clearance <30 mL/min). |
Usually started by a specialist following an episode of spontaneous bacterial peritonitis in patients with persistent ascites. Proton pump inhibitors can increase the risk of spontaneous bacterial peritonitis. |
|
Non-absorbable disaccharides: • lactulose |
Treat and prevent recurrence of hepatic encephalopathy. Acidify the gut and promote healthy gut flora (prebiotic), thereby reducing production and absorption of ammonia. |
Contraindicated: intestinal obstruction. |
In patients with genuine intolerance to lactulose, macrogol-containing laxatives can be used. Usually titrated to achieve 2–3 loose bowel motions each day. |
|
Non-absorbable antibiotics: • rifaximin |
Prevent recurrent hepatic encephalopathy. Modify gut flora and reduce production of ammonia. |
Contraindicated: intestinal obstruction. Caution: Child-Pugh C cirrhosis (increased systemic activity). |
Must be started by (or in consultation with) a gastroenterologist or hepatologist. Use concomitantly with lactulose if tolerated. |
PBS Pharmaceutical Benefits Scheme
In heavy drinkers who suddenly discontinue or decrease alcohol consumption, benzodiazepines may be used short term with other supportive measures to manage withdrawal symptoms.28 The Clinical Institute Withdrawal Assessment for Alcohol Revised (CIWA-Ar) Score32 can assist the evaluation of alcohol withdrawal syndrome severity and benzodiazepine requirements. Patients with moderate or severe alcohol withdrawal syndrome are usually managed in hospital, but small doses of benzodiazepine may be continued for a short duration on discharge. Diazepam is usually preferred because of its long half-life, although oxazepam may be safer in cirrhosis.28
Outside the setting of alcohol withdrawal, benzodiazepines are potentially inappropriate. They should be prescribed with extreme caution (especially in cirrhosis) as the risk of adverse effects may outweigh the benefits. The decision to prescribe benzodiazepines in alcohol-associated liver disease should be made on a case-by-case basis as patients may be at increased risk of harm due to pharmacodynamic interactions. Benzodiazepines have also been associated with an increased risk of first-time hepatic encephalopathy in cirrhosis when taken for 3–10 days.29
Alcoholic hepatitis can be a life-threatening condition associated with heavy alcohol use. It usually presents with jaundice and a characteristic pattern of liver biochemistry (Table 1).9,17 Symptoms can include fever, right upper-quadrant or epigastric pain and tenderness, and occasionally ascites or hepatic encephalopathy. Infection and sepsis are relatively common and severe complications of alcoholic hepatitis leading to poor outcomes.22 Mortality associated with alcoholic hepatitis is high and immediate referral to hospital for assessment, support and treatment is essential.9,16
Treatment of alcoholic hepatitis focuses on nutritional support and complete abstinence from alcohol. In severe cases corticosteroids may be considered, although evidence for their effectiveness remains inconclusive.33 Patients may be discharged with oral prednisolone to complete a 28-day course, followed by an optional three-week taper.22 Following discharge from hospital, GP review and timely cessation of temporary concomitant therapies such as proton pump inhibitors may be helpful to prevent inappropriate long-term use. Re-introduction of temporarily withheld medications (e.g. nephrotoxic drugs including diuretics, ACE inhibitors and sartans) can be considered when renal function has stabilised.
Malnourishment is prevalent in alcohol-associated liver disease due to poor oral intake, hypermetabolism, altered nutritional requirements and malabsorption of fats.34 Correction of pancreatic insufficiency (e.g. pancreatic enzyme replacement) and nutritional support may be required to maintain muscle mass and prevent catabolism (energy intake 25–40 kcal/kg/day and protein intake 1–1.5 g/kg/day).34,35 Multivitamins and supplements to correct specific deficiencies are also commonly used in clinical practice.
In all stages of alcohol-associated liver disease, vitamin B1 (thiamine) supplementation is strongly recommended to prevent neurological complications like Wernicke-Korsakoff’s syndrome.31 If Wernicke-Korsakoff’s syndrome is suspected (e.g. acute confusion, delirium), immediate referral to hospital is required. Vitamin B12 supplementation is also recommended in deficiency to prevent neuropathies and megaloblastic anaemia.31
Supplementation of fat-soluble vitamins (A, D, E and K) is not routinely recommended, except for vitamin D deficient patients with cirrhosis or bone disease.25,31 The benefits of supplementing other micronutrients including ascorbic acid, magnesium and selenium are debated and they are not routinely recommended in clinical practice. Antioxidants including beta-carotene, vitamin A, vitamin C, vitamin E and selenium have been trialled to reduce oxidative stress and liver damage. However, a Cochrane review found no evidence to support these supplements in patients with liver disease.36
Progression of liver disease in the setting of ongoing alcohol consumption and other risk factors can lead to cirrhosis (Fig.). These patients may experience asymptomatic disease (‘compensated’) or present with complications of portal hypertension and liver insufficiency (‘decompensated’).26,37 All patients with suspected cirrhosis should be referred for specialist evaluation.
Cirrhosis can potentially reduce clearance and increase exposure to certain drugs or metabolites38 due to:
Consequently, people with cirrhosis are at greater risk of experiencing adverse drug reactions compared to those with non-cirrhotic liver disease.39 This is especially the case for patients with complications like ascites, hepatic encephalopathy, jaundice and variceal bleeding who are at higher risk of pharmacodynamic interactions.
Practical prescribing recommendations for individual medicines (based on pharmacokinetic changes) are available to guide drug selection and dose adjustments for people with cirrhosis.40,41 Progression to Child-Pugh B/C cirrhosis increases the likelihood of pharmacokinetic changes and pharmacodynamic interactions,41 especially among potentially inappropriate medicines (Table 3).15,18,20,21,29,40-44 Even medicines that are regularly used to manage the complications of cirrhosis such as diuretics, lactulose and non- selective beta blockers require regular titration and monitoring to prevent medication-related harm due to pharmacodynamic changes (e.g. dehydration, electrolyte derangement, hypotension).
Table 3 - Potentially inappropriate medicines in alcohol-associated liver disease15,18,20,21,29,40-44
|
Drug |
Stage to avoid use |
Medication safety considerations |
|
ACE inhibitors and sartans: • e.g. ramipril, perindopril, irbesartan, telmisartan |
Alcoholic hepatitis Cirrhosis Especially patients with ascites or renal impairment |
Increased risk of interactions with increasing severity of liver disease due to progressive alteration in renal haemodynamics. Commence at a low dose and titrate slowly. The risk of harm in Child-Pugh C cirrhosis may outweigh benefits. |
|
Antibiotics: • metronidazole, nitrofurantoin, sulfamethoxazole |
Alcohol use disorder |
Interaction with alcohol may lead to disulfiram-like reactions (nausea, vomiting, flushing, headache, palpitations). Patients should avoid consuming alcohol during treatment and for 24 hours after finishing the course. Nitrofurantoin may cause drug-induced liver injury. |
|
Antiplatelets and anticoagulants: • e.g. ticagrelor, dabigatran, rivaroxaban |
Cirrhosis (varies by drug class) |
Standard markers of haemostasis (INR, prothrombin time, platelet count) do not accurately reflect coagulative status. Low-molecular-weight heparins and vitamin K antagonists are preferred to manage venous thromboembolism. Limited experience with direct-acting oral anticoagulants. Avoid use in advanced cirrhosis. Clopidogrel and prasugrel appear safe in Child-Pugh A and B cirrhosis. Safety of ticagrelor in advanced cirrhosis is unknown. Aspirin appears safe. |
|
Benzodiazepines: • e.g. diazepam, oxazepam, temazepam |
Alcohol use disorder Cirrhosis Especially patients with history of hepatic encephalopathy |
Alcohol consumption enhances the sedative effect of benzodiazepines including drowsiness, sedation and impaired motor skills. Even short-term use can precipitate hepatic encephalopathy. If a benzodiazepine is indicated, oxazepam or temazepam are preferred due to the comparatively simple hepatic metabolism. |
|
Calcium channel blockers: • e.g. felodipine, lercanidipine, verapamil |
Cirrhosis Especially patients with symptomatic hypotension or those co-prescribed non-selective beta blockers |
If a calcium channel blocker is indicated, amlodipine, nifedipine and diltiazem appear safe if commenced at a low dose and titrated slowly. Felodipine, lercanidipine and verapamil should be avoided in Child-Pugh C cirrhosis. |
|
Non-steroidal anti-inflammatory drugs: • e.g. ibuprofen, diclofenac, celecoxib |
Alcohol use disorder Alcoholic hepatitis Cirrhosis Especially patients with ascites or renal impairment |
Alcohol consumption increases the risk of peptic ulcer disease and gastrointestinal bleeding. Increased risk of renal impairment, acute kidney injury and hepatorenal syndrome in acute and chronic hepatic impairment. All non-steroidal anti-inflammatory drugs should be avoided. Paracetamol is a safe alternative (maximum 2–3 g daily in malnourished patients and those with cirrhosis). |
|
Opioids: • e.g. oxycodone, tramadol, morphine, tapentadol |
Alcohol use disorder Cirrhosis Especially patients with history of hepatic encephalopathy |
Alcohol consumption enhances the sedative effect of opioids including drowsiness, sedation and impaired motor skills. May precipitate hepatic encephalopathy, especially in patients not taking appropriate laxatives. All slow-release formulations (especially patches) should be avoided due to reversal difficulties if hepatic encephalopathy occurs. If an opioid is indicated, immediate-release tramadol or oxycodone appear safe if commenced at a low dose and titrated slowly. Use paracetamol as an opioid-sparing drug. Avoid tapentadol in Child-Pugh C cirrhosis. |
|
Proton pump inhibitors: • e.g. pantoprazole, rabeprazole, omeprazole |
Nutritional deficiency Cirrhosis Especially patients with ascites, history of hepatic encephalopathy, or recurrent infections |
Inhibition of gastric acid secretion alters bioavailability and absorption of vitamins and minerals. If a proton pump inhibitor is indicated, (es)omeprazole and rabeprazole appear safe at low doses. Esomeprazole may be safest in Child-Pugh C cirrhosis. People with cirrhosis often have impaired immunity. Inhibition of gastric acid secretion further increases infection risk, especially spontaneous bacterial peritonitis and Clostridium difficile infection. |
|
Oral hypoglycaemic drugs: • e.g. metformin, sulfonylureas, dipeptidyl peptidase-4 inhibitors, sodium-glucose co-transporter 2 inhibitors, pioglitazone |
Cirrhosis (varies by drug class) |
Metformin has a favourable safety profile and numerous benefits in chronic liver disease. There is conflicting evidence about the risk of lactic acidosis in advanced cirrhosis. Avoid sulfonylureas in cirrhosis due to the risk of hypoglycaemia. Avoid pioglitazone in advanced cirrhosis. Limited experience with dipeptidyl peptidase-4 inhibitors and sodium-glucose co-transporter 2 inhibitors in cirrhosis. Dose reduction is often required. Avoid use in advanced cirrhosis. |
While the comorbidity burden is often lower in alcohol-associated liver disease compared to other types of chronic liver disease (e.g. non-alcoholic fatty liver disease), the prevalence of hypertension (32–41%), ischaemic heart disease (5–20%), heart failure (5–12%) and type 2 diabetes (26–29%) is notable.45,46 Concomitant drugs prescribed for these conditions may require additional monitoring, especially in people with cirrhosis. In those with decompensated cirrhosis who are ineligible for liver transplant, deprescribing medicines for which benefit is with long-term use (e.g. statins) could be considered. This will reduce the medication burden for these patients who will likely follow a palliative course, with a median survival of approximately two years.37
Doctors, nurses, and pharmacists in the primary care setting have an important role in the management of patients with alcohol-associated liver disease. In addition to supporting abstinence, optimising medicine use is imperative to improve outcomes and minimise harm.
Conflicts of interest: Kelly Hayward was supported by a Health Innovation, Investment and Research Office (HIIRO) Clinical Research Fellowship.
Australian Prescriber welcomes Feedback.
Hepatology research fellow, Centre for Liver Disease Research, Faculty of Medicine, Translational Research Institute, The University of Queensland, Brisbane
Hepatology research fellow, Department of Gastroenterology and Hepatology, Princess Alexandra Hospital, Brisbane
Clinical research fellow, Centre for Liver Disease Research, Faculty of Medicine, Translational Research Institute, The University of Queensland, Brisbane
Liver disease pharmacist, Department of Gastroenterology and Hepatology, Princess Alexandra Hospital, Brisbane

