Diagnostic tests
The role of cardiac imaging in clinical practice
- Michael Benjamin Stokes, Ross Roberts-Thomson
- Aust Prescr 2017;40:151-5
- 1 August 2017
- DOI: 10.18773/austprescr.2017.045
The selection of cardiac imaging modality depends on the indication, individual patient characteristics and local accessibility.
In many cases echocardiography, including stress echocardiography, can provide the required clinical information and avoids radiation exposure.
CT coronary angiography is increasingly used to detect coronary artery disease in patients with an intermediate risk and in those with equivocal stress test results.
Cardiac MRI studies are ordered by a patient’s cardiologist as an adjunct to other imaging modalities when further clarification is warranted.
A variety of clinical presentations including dyspnoea, chest pain, syncope and palpitations may arouse suspicion of cardiovascular disease. Following a clinical history and examination, imaging of the heart may be required. Cardiac imaging is also used to monitor patients with known pathology in many cardiovascular diseases such as interval monitoring of aortic stenosis.
The choice of cardiac imaging modality depends on the disease being investigated, individual patient characteristics and the accessibility of tests. Assessment of dyspnoea and investigation for coronary artery disease are two of the most common clinical scenarios that may require cardiac imaging. Imaging is also indicated in the diagnosis of cardiomyopathy, and structural or congenital heart disease.
If a cardiac aetiology is suspected, a targeted investigative approach with clinical follow-up is prudent to ensure correct diagnosis and appropriate specialist referrals.
Chest X-ray has a role in the preliminary assessment of cardiovascular disease. An increase in heart size and the presence of increased pulmonary vascular markings or pleural effusions may indicate pulmonary congestion secondary to cardiac failure. A chest X-ray may also help exclude pulmonary pathology such as infection, malignancy or fibrosis. Importantly, a normal chest X-ray cannot reliably exclude cardiac aetiology in a patient presenting with dyspnoea. It may not show significant pathologies including valvular heart disease and pulmonary arterial hypertension.
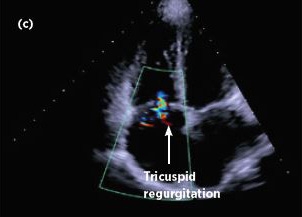
Transthoracic echocardiography has many uses (see Box) and is relatively accessible. It can be extremely useful for evaluating dyspnoea. In many cases it provides structural and functional information that indicates a particular diagnosis (see Fig.).
Echocardiography can provide diagnostic information in suspected cases of cardiac failure and in the diagnosis of valvular heart disease when a patient is found to have a murmur that warrants investigation. Congenital heart disease such as septal defects can be identified on echocardiography. Echocardiography can also provide a non-invasive estimation of pulmonary arterial systolic pressure and identify other features consistent with the presence of pulmonary arterial hypertension.
A limitation of echocardiography is the difficulty in obtaining interpretable ultrasound images in some patients. For example, in those with obesity or lung disease (like emphysema) the ability of echocardiographic images to be transmitted across air-space is compromised due to increased lung volumes.

|

|
|
|
 |

|
(a) Left ventricle chamber measurement in the parasternal long-axis view
(b) Colour doppler demonstrating central aortic regurgitation
(c) Tricuspid regurgitant jet evident on colour doppler imaging
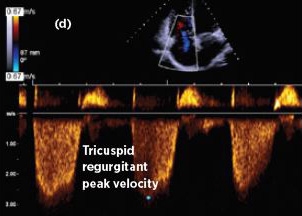
(d) Peak velocity of the tricuspid regurgitant jet (used to estimate pulmonary artery systolic pressure) – this is unable to be adequately detected in approximately 30% of patients undergoing echocardiography
e) Video demonstrating a dilated left ventricle with severe left ventricular dysfunction
f) Video demonstrating a case of hypertrophic cardiomyopathy with markedly increased myocardial wall thickness, systolic anterior motion of the mitral valve and dynamic left ventricular outflow tract obstruction
When initial cardiac imaging is non-diagnostic or inconclusive and respiratory conditions have been excluded, coronary artery disease should be considered.
Stress ECG is a cheap, safe and accessible test but it has low sensitivity and specificity for coronary artery disease, and therefore has a limited role in evaluating patients with chest pain. It can be used for assessing low-risk patients who present to an emergency department with chest pain when acute coronary syndrome has been excluded. It also has a limited role in patients with known coronary artery disease to assess symptom control with medical therapy and can help to identify those who may benefit from augmented anti-anginal therapy or coronary revascularisation.2,3
Stress echocardiography provides an effective, non-invasive assessment of patients with chest pain. The added structural and functional information gained from this test can often be very useful. It is generally accessible and diagnostically reliable. Compared with nuclear stress perfusion studies, it avoids radiation exposure, has greater specificity and is substantially less costly to the public health system. It can be performed using a bicycle or treadmill, or with pharmacological stress (e.g. with dobutamine) in those unable to exercise.
CT coronary angiography directly visualises the coronary arteries for both non-obstructive and obstructive coronary artery disease. Thus, it is considered a highly effective first-line investigation in patients with a low–intermediate predicted risk of coronary artery disease.2 However, it does not tell the physician whether a coronary stenosis is haemodynamically significant, which requires a functional study such as stress echocardiography or nuclear stress perfusion. Detection of coronary plaque via CT coronary angiography may help to determine whether medical therapy such as long-term statins are indicated.
CT coronary angiography is also very useful for patients with an equivocal result from a stress test. Radiation exposure is lower than with invasive coronary angiography and nuclear stress perfusion testing. CT is also significantly less expensive and avoids the small associated risks of invasive coronary angiography. A heart rate of 60 beats per minute or less is required to optimise image quality for adequate interpretation. Temporary oral and intravenous beta blockers in combination with ivabradine are used to achieve this.
Detection and quantification of coronary artery calcification using multidetector computer tomography has emerged as a technique that may predict the risk of future cardiovascular events in individuals at intermediate risk of coronary artery disease. The degree of calcification can be quantified (via a score) and the patient’s burden can be graded into age-specific quartiles. Multiple, large observational studies have shown that those with significantly elevated scores are at greater risk of myocardial infarction. The absence of calcification is also highly predictive of the absence of significant coronary stenosis and confers a favourable cardiac prognosis.4
Calcification scores have no role in the evaluation of patients presenting with chest pain. Its use is reserved for assessing the risk of future cardiac events and to guide clinicians about whether primary prevention of ischaemic heart disease with statin therapy is appropriate. This is reserved for patients with an intermediate risk determined using a risk calculator such as the Framingham Risk Score.4 Despite data from numerous observational studies, improvement in cardiovascular outcomes in those who take primary prevention therapy in the context of an elevated calcification score remains contentious.4
Nuclear stress perfusion has a role in the evaluation of chest pain in specific clinical settings such as patients with bundle branch blocks, poor echocardiographic images and in those with previous myocardial infarction or previous coronary artery bypass surgery. Local availability of other tests may also necessitate its use.
Similar to stress echocardiography, nuclear stress perfusion can be performed with exercise or drugs. The indications for a nuclear stress perfusion study are similar to stress echocardiography. However, because of its higher cost, radiation exposure and lower specificity, nuclear stress perfusion is reserved for when stress echocardiography cannot be interpreted or is unavailable.
Transoesophageal echocardiography and cardiac MRI have a role in a number of clinical scenarios and are useful adjuncts when there is not enough other diagnostic information.
Transoesophageal echocardiography is generally performed with both local (oral lidocaine (lignocaine) topical spray) and intravenous anaesthesia.
It is useful for:
When assessing congenital heart disease, transoesophageal echocardiography can overcome many of the limitations of transthoracic echocardiography in delineation and visualisation of cardiac chambers, intra-cardiac shunts and in the monitoring of patients with previous surgery. Examples of its use in congenital heart disease include identifying and quantifying atrial septal defects and anomalous pulmonary venous drainage, and detecting the complications of previous corrective surgery for congenital heart disease.
Cardiac MRI is very specialised and access is limited. In Australia, cardiologists request cardiac MRI when additive information to other testing is required. The only current indications with a Medicare rebate are the assessment of a cardiac mass, congenital heart disease and in bicuspid aortic valve disease.5 It is useful in bicuspid aortic valve disease for detecting and monitoring associated aortopathy, detecting the presence of aortic coarctation and in quantifying the severity of aortic regurgitation by measuring regurgitant volumes.
Cardiac MRI avoids the repeated radiation exposure of CT in those requiring interval studies. However, it has a number of important contraindications and completion of an MRI safety questionnaire is required before undertaking a study. Contraindications include patients with metallic implants (such as aneurysm clips and neurostimulators) and those with an implanted cardiac pacemaker or defibrillator. However, a growing number of cardiac devices are now considered to be compatible with MRI (termed MRI-conditional).6
Cardiac MRI may be useful in the following cardiomyopathies:
Cardiac MRI is the imaging modality of choice to diagnose myocarditis by detecting myocardial inflammation and myocardial oedema using a number of specific MRI sequences.7
Thorough clinical assessment before requesting cardiac imaging is crucial in formulating a differential diagnosis so that the appropriate test is requested and the imaging study can be targeted effectively.
Cardiac imaging is an integral aspect in the diagnosis and monitoring of cardiovascular disease. CT coronary angiography and cardiac MRI are both relatively recent in their clinical use compared to echocardiography and nuclear cardiac studies, but both provide extremely valuable and additive information to other modalities when used appropriately.
Conflict of interest: none declared

Fellow in Cardiac Imaging, Cardiology, Royal Adelaide Hospital, Adelaide
Advanced trainee, Cardiology, Royal Adelaide Hospital, Adelaide
