Abnormal laboratory results
Troponins in myocardial infarction and injury
- Julia M Potter, Peter E Hickman, Louise Cullen
- Aust Prescr 2022;45:53-7
- 1 April 2022
- DOI: 10.18773/austprescr.2022.006
Troponins are proteins that are integral components of the contractile mechanism of muscle, including cardiac muscle. Cardiac troponins I and T can be detected in the blood of most people after puberty, at concentrations reflecting cardiac mass, sex and age.
Current laboratory assays are approximately 1000 times more sensitive than those used previously. They also have higher sensitivity than point-of-care assays.
The measurement of cardiac troponins is used primarily to assist in the diagnosis or exclusion of myocardial injury. Serial tests in acute coronary syndrome are guided by the Universal Definition of Myocardial Infarction.
Troponins are proteins that regulate muscle contraction.1 In the myocardium the subunits are cardiac troponin I (cTnI), cardiac troponin T (cTnT) and cardiac troponin C. All three are integral components of the contractile mechanism of cardiac muscle (see Fig. 1). They have separate genes, which differentiate them from skeletal muscle troponin.
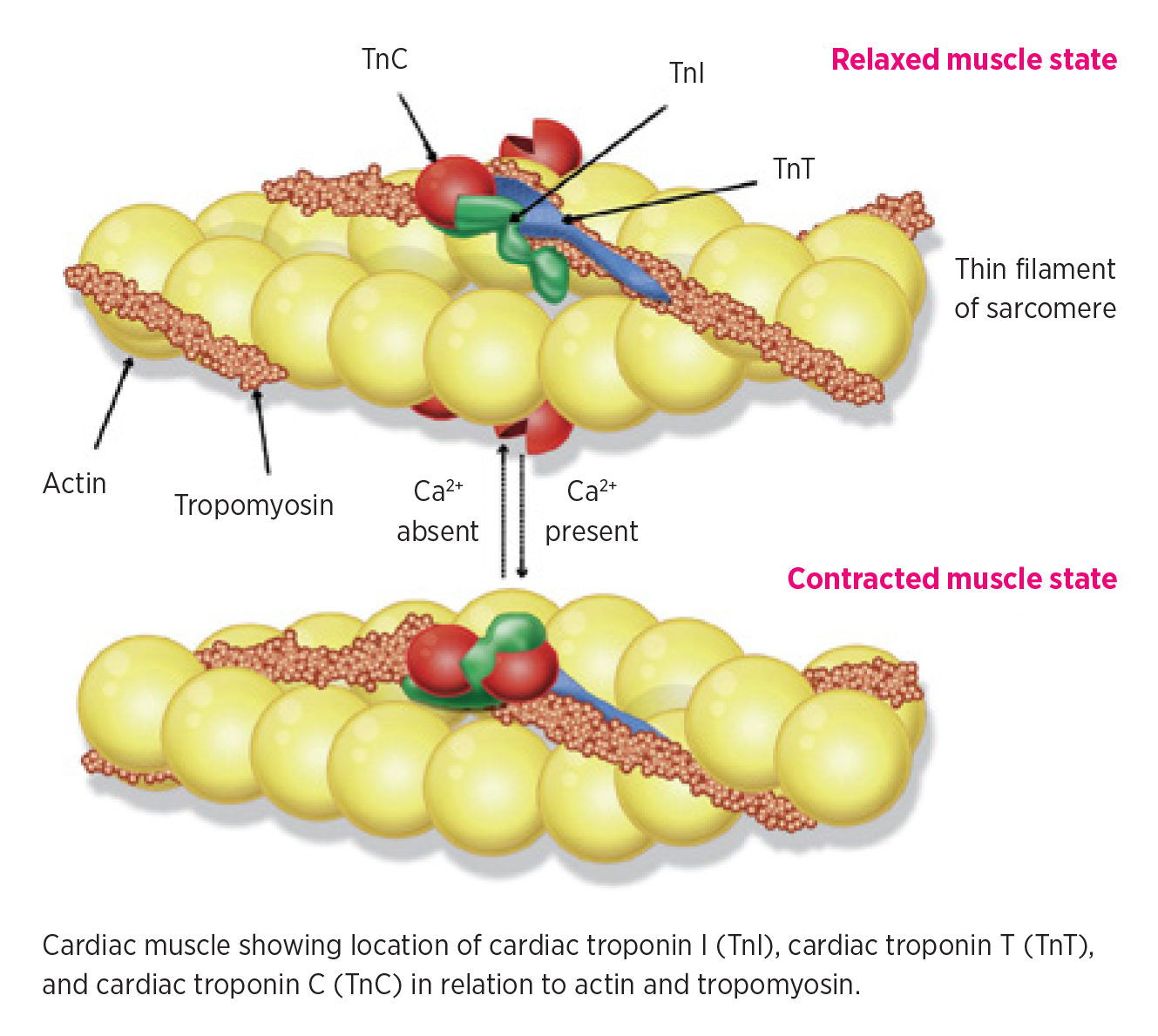
Ca2+ Calcium ions
Source: Adapted, with permission from Elsevier, from reference 1.
Immunoassays have been developed for both cTnI and cTnT and either of these troponins can be used in the investigation of possible myocardial injury or infarction. As cardiac troponins are specific for myocardial tissue, they have now replaced creatine kinase-MB for investigating possible myocardial injury.
Early assays for cTnI and cTnT were relatively insensitive. Only high concentrations could be detected in the circulation. This led to the concept that troponin release from the myocardium only occurred after significant ischaemic damage. The detection of troponins in the blood became almost synonymous with acute coronary syndrome. However, newer assays are approximately 1000-fold more sensitive so they can detect troponins in people without ischaemia. Low concentrations can be detected in the circulation in healthy people throughout life, and almost all children from near puberty have detectable cTnI in their blood.2 Plasma concentrations are lower in females than males because of their smaller cardiac mass. Many causes of myocardial damage other than ischaemia are associated with troponin elevations in the circulation and high concentrations can occur in marathon runners (Box 1).3-6 The diagnosis or exclusion of acute coronary syndrome remains the most common and important reason for measuring troponins.
For technical reasons (namely the sample volume used) cTnI assays measure to lower concentrations than cTnT. However, in the diagnosis of myocardial infarction there is little difference between cTnT and cTnI. An exception is in patients undergoing haemodialysis, where cTnT is marginally superior in identifying those at risk of cardiac death.9 Whether a particular laboratory measures cTnI or cTnT will depend on the analytical equipment it has chosen. Only one company offers cTnT, whereas multiple platforms offer cTnI assays.
All troponin assays offered in major hospital and pathology laboratories in Australia are high-sensitivity assays. However, the concentrations measured by different assays are not interchangeable. The equipment manufacturers have not benchmarked their particular antibodies against each other and there has been no harmonisation of the immunoassays. This means that the reference intervals reported by different laboratories will vary.
Some small laboratories and geographically more remote locations are unable to support significant large instrumentation and rely on point-of-care testing for troponin. While these tests are generally robust, their limits of detection are higher. For example, the limit of detection for cTnI may be 20 nanogram/L compared with 2 nanogram/L for a high-sensitivity assay.10 For measuring cTnT using the point-of-care testing, the limit of detection is 100 nanogram/L versus 5 nanogram/L for a high-sensitivity assay.11 As significant myocardial injury can occur with troponin concentrations below the limits of detection, some cases of concern may be missed by point-of-care tests. High-sensitivity point-of-care assays are in development, but are not currently in use in Australia.
The Fourth Universal Definition of Myocardial Infarction (Box 2) requires a rise and fall in troponin concentration with at least one result above the 99th percentile, and objective evidence of myocardial ischaemia.12 The most common form of acute coronary syndrome seen in the emergency department is type 1 myocardial infarction. This is caused by the rupture of an atheromatous plaque, thrombi formation and embolisation causing coronary artery obstruction and necrosis. Type 2 myocardial infarction occurs when oxygen delivery to the myocardium is inadequate.13 Other types of myocardial infarction are rare.
The universal definition uses the 99th percentile of troponin concentrations in a healthy population. This is challenging as defining a healthy population is difficult. Detailed examination shows many apparently healthy people have significant sub-clinical cardiac disease. Depending on how carefully a population is chosen, the reported 99th percentile can vary markedly.14 In addition, both sex and age (increase with age) are important contributors to population data sets even in a carefully selected population.15 In Australia the 99th percentiles (depending on the assay used) are:
The universal definition introduced the 99th percentile to assist the recognition of clinically important elevations of cardiac troponin. However, it is important to recognise that with the very small biological variation of both cTnT and cTnI in healthy individuals these concentrations may fall well below the 99th percentile. A pathologically significant troponin release can therefore occur and still be below the 99th percentile in some individuals.16
The single major use of troponin assays is for the diagnosis or exclusion of acute myocardial infarction in the emergency department. Only 5–10% of people who are assessed are ultimately proven to have a myocardial infarction.17 Troponin is therefore mainly used in the emergency department as a ‘rule-out’ test. A low troponin concentration at presentation with small changes over a period of 1–3 hours provides the best rule-out rates.18 Sex-specific cutpoints are recommended for use by both the Fourth Universal Definition of Myocardial Infarction and the current guidelines of the National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand.19 Using these different cutpoints has increased the diagnosis of acute coronary syndrome in females.20
Particularly in the early days of troponin testing, cardiologists were concerned over the large numbers of patients referred with small increases in troponin unrelated to acute coronary syndrome or acute myocardial infarction. In attempting to reduce these ‘false positives’, the 99th percentile was introduced as a diagnostic criterion, making troponin a ‘rule-in’ test.21
In myocardial infarction there is an acute change in troponin concentration, however, patients may present days after their initial chest pain. Concentrations of cTnI may remain elevated for up to 4–5 days and cTnT up to 10 days, but two samples collected 2–3 hours apart may not be significantly different.
Troponin testing in general practice is not encouraged, as the troponin concentration alone does not rule out acute coronary syndrome.19 A definitive risk stratification (with more than just a single measurement) is required. There are exceptions to this in rural or remote settings, or in patients presenting several days after symptom onset.
Cardiac troponins are measured by immunoassays which are prone to interference by endogenous immunoglobulins. They may bind to either of the troponins, or to the exogenous antibodies that are used in the assays. These interferences can be either positive or negative. If a troponin result does not fit with a strong clinical impression, talk to the laboratory about possible investigations for interference.22
A raised troponin concentration may be a sign of myocardial injury rather than infarction. Figure 2 shows the relative time courses of the major cardiac causes of chest pain including acute myocardial infarction. The shared pathway for myocardial damage is either an absolute or relative insufficiency of oxygen availability to meet myocardial requirements (Box 1). Elevated cardiac troponins in pulmonary embolism and in heart failure identify high-risk patients, but do not significantly influence management. In all conditions investigated to date, an elevated cardiac troponin is associated with a poorer prognosis in adults23 and children.24
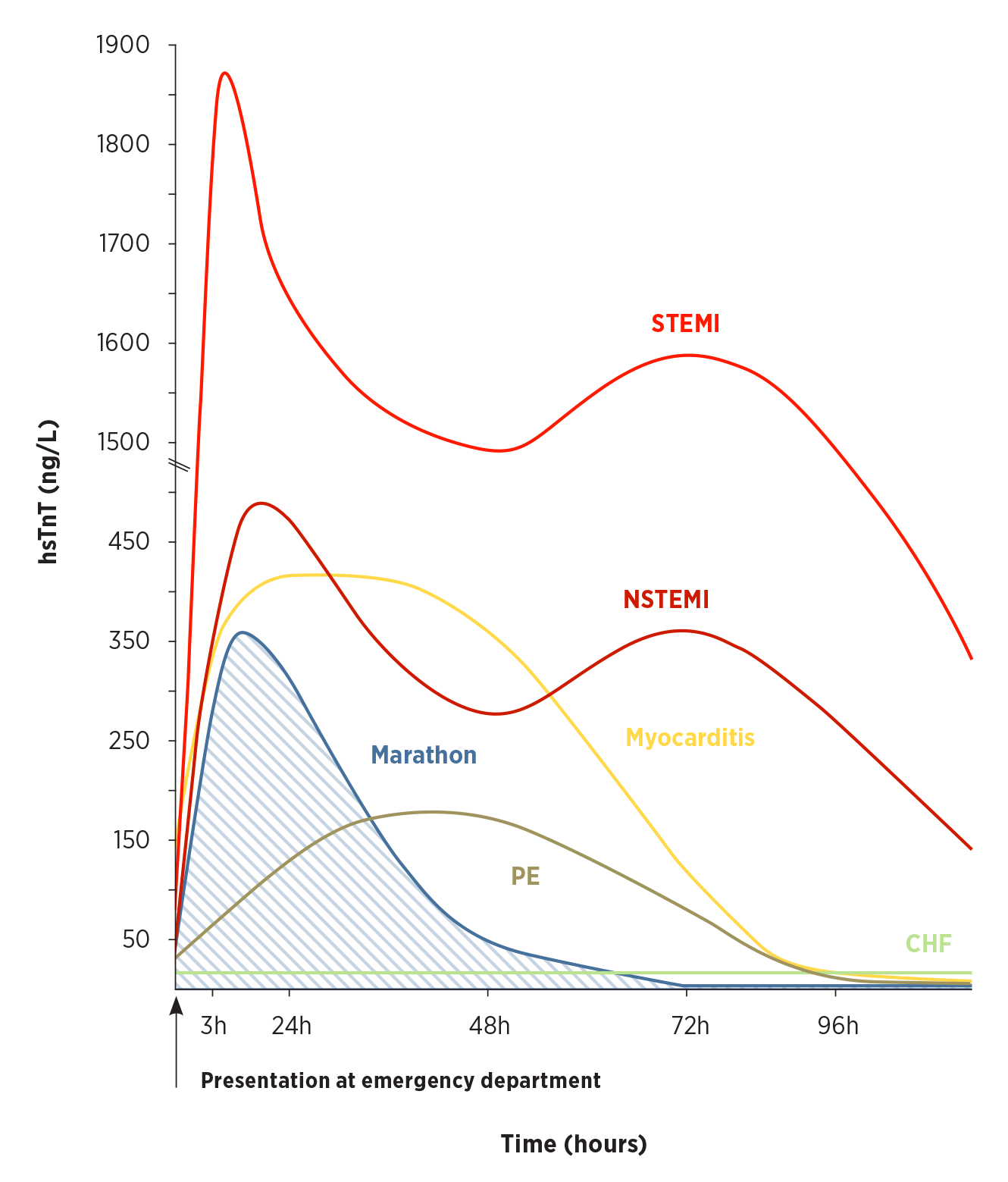
Cardiac troponin T kinetics for ST-elevation myocardial infarction (STEMI) and non- ST-elevation myocardial infarction (NSTEMI) are typically biphasic compared to monophasic kinetics in myocarditis, pulmonary embolism (PE), and endurance sports. The concentration of high-sensitivity troponin T measured can vary markedly after a marathon run (shaded area) and can even supersede that of, for example, NSTEMI.
In chronic heart failure (CHF) troponin concentrations are persistent and often not elevated in the absence of an ischaemic episode.
hsTnt high-sensitivity cardiac troponin T concentration
Although some drugs used in chemotherapy are cardiotoxic,25 routine monitoring with troponins has not been adopted to identify patients at risk. In contrast, monitoring for the early transient cardiotoxicity which can occur when starting clozapine is more common.4
The finding of an unexpected elevated cardiac troponin requires explanation and clinical evaluation. For conditions in which the underlying cause is a mismatch of oxygen supply and demand, the expectation is a rise then fall in cardiac troponin (Fig. 2).26 Compare this with drug-related causes where the changes may occur over a different timeframe and depend on the mechanism of damage and clearance of the drug. In chronic conditions such as end-stage renal failure, the troponin concentrations remain elevated, but are reversed following renal transplantation.
The measurement of cardiac troponins has a role in the diagnosis of acute coronary syndrome. However, many other conditions cause a rise in troponin concentrations. The importance of troponin in the diagnosis of acute coronary syndrome should, to some extent, be de-emphasised, with more weight given to the clinical presentation of the individual patient. It is a synthesis of clinical examination, ECG assessment, cardiac troponin measurement and imaging that may be needed to make the diagnosis of acute coronary syndrome.27
Health professionals need to be aware of the factors that can affect the results of troponin assays. A raised troponin concentration may be a sign of myocardial injury rather than infarction.
Conflicts of interest: none declared
This article is peer-reviewed.
Australian Prescriber welcomes Feedback.
Fraser CG. Biological variation: from principles to practice. Washington, DC: AACC Press; 2001.
Emeritus professor, Australian National University Medical School, Canberra
Hon visiting medical officer, Canberra Hospital
Associate professor, Australian National University Medical School, Canberra
Visiting medical officer, Canberra Hospital
Senior staff specialist, Emergency and Trauma Centre, Royal Brisbane and Women’s Hospital

