Medicinal mishap
Bisphosphonates and osteonecrosis of the jaws
- Alastair Goss, Patricia Backhouse
- Aust Prescr 2007;30:96-7
- 1 August 2007
- DOI: 10.18773/austprescr.2007.058
An otherwise well 66-year-old woman was referred with pain, swelling and numbness of the left mandible with pus discharging from around a dental implant. Her problems had developed over the previous six months.
The patient had undergone dental reconstruction 15—20 years previously. This involved eight titanium implants in both jaws with extensive crown and bridge work. (This work involved a personal cost of approximately $25 000 above insurance benefits.)
The woman had been diagnosed with 'borderline osteoporosis'. Her bone mineral density was —2.42 standard deviations below normal (consistent with a diagnosis of osteopenia). She was prescribed 70 mg alendronate weekly but later developed stress fractures. Over three years she took a total dose of 11.2 g.
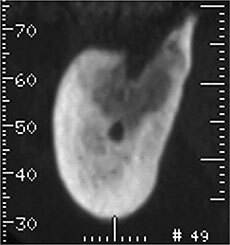
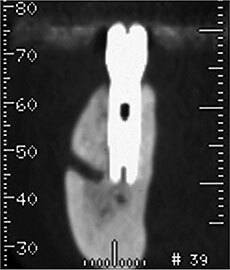
A clinical diagnosis of bisphosphonate-associated osteonecrosis of the left mandible was made. A CT scan showed extensive involvement around the infected implant. The right mandible and maxilla were not involved.
Alendronate was ceased and non-surgical treatment commenced with 0.12% chlorhexidine mouth washes, intermittent short courses of cephalosporins for the soft tissue infection, and tramadol or paracetamol with codeine for the pain. This controlled the acute symptoms.
One year after stopping alendronate the symptoms recurred. A repeat CT scan showed extension of the necrosis without bone reformation. The involved implant and soft tissue were curetted under general anaesthesia. The wound healed slowly (see Fig. 1).
In this case alendronate was commenced before bisphosphonate-associated osteonecrosis of the jaw had been described.1Osteonecrosis associated with a previously stable implant was one of the first such presentations in Australia.
Bisphosphonate-associated osteonecrosis of the jaws is now defined as an area of exposed bone in the jaws which persists for more than eight weeks. Other conditions, including osteoradionecrosis and the presence of tumour, need to be excluded. The first described cases were in older, medically compromised patients treated with intravenous infusions of potent nitrogen containing bisphosphonates for multiple myeloma, breast or prostatic metastasis or malignant hypercalcaemia.2The most commonly reported drugs involved were zoledronic acid followed by pamidronate.3,4Common triggers for osteonecrosis of the jaws were dental extractions, periodontal disease or oral trauma. The frequency of osteonecrosis of the jaws following dental extractions in oncology patients was 1—10%. It is a painful and persistent condition which represents another difficulty that confronts patients with cancer.
This case shows a different situation as it involved two common benign conditions, osteopenia and dental disease. Approximately three million prescriptions were written for oral bisphosphonates last year, and 10% of all Australians have a dental extraction in any given year. Although the risk of osteonecrosis of the jaws after dental extraction is low (0.1—0.3%) for a patient on oral bisphosphonates for osteoporosis, the potential number of cases is high.3It is anticipated that the number will increase as the population ages and the number of prescriptions and duration of bisphosphonate dosage increases. Osteonecrosis of the jaws is uncommon in patients who have taken oral bisphosphonates for less than three years.
Just as an extraction requires bone turnover to heal, dental implants require bone turnover to maintain osseointegration. The frequency of osteonecrosis of the jaws associated with dental implants is unknown.
Strategies to minimise the risk of osteonecrosis of the jaws with bisphosphonates are unclear. It is important to ensure that the patient has good oral health. This should be regularly assessed by a dentist.
CT of mandible
|
|||||||||||||||||
Clinicians who treat osteoporosis with bisphosphonates need to balance the known beneficial effects of treatment with the small risk of osteonecrosis of the jaws. This risk can be minimised by ensuring that the patient is dentally fit and, in particular, does not require dental extractions or other jawbone surgery, including dental implants.
Oral and Maxillofacial Surgeon, Adelaide
General Practitioner, Adelaide