Article
Chronic heart failure
- Ingrid Hopper, Kellie Easton
- Aust Prescr 2017;40:128-36
- 1 August 2017
- DOI: 10.18773/austprescr.2017.044
The clinical diagnosis of heart failure should be confirmed by echocardiogram to determine the underlying mechanism and to measure the left ventricular ejection fraction. Heart failure with reduced ejection fraction and heart failure with preserved ejection fraction have different treatments but are often indistinguishable clinically.
Lifestyle modification and education on self-management are important strategies for all patients. Patients should monitor their symptoms and weight regularly.
Heart failure with reduced ejection fraction should be managed with ACE inhibitors, heart failure specific beta blockers, and aldosterone antagonists. These drugs all reduce mortality.
Angiotensin receptor antagonists should be used if the patient cannot tolerate ACE inhibitors. The combination of sacubitril and valsartan is indicated if patients remain symptomatic despite ACE inhibitors, beta blockers and aldosterone antagonists. Digoxin and diuretics may also have a role in treating persistent symptoms.
In heart failure with preserved ejection fraction no drug has been proven to reduce mortality. Patients should be treated cautiously with diuretics and have aggressive management of risk factors, particularly hypertension.
Heart failure is present in 1–2% of the Australian population.1 It is predominantly a disease of the elderly,2 present in up to 10% of those aged over 80,3 and this prevalence is rising.4
Heart failure is a syndrome in which the heart cannot provide adequate cardiac output to meet the metabolic requirements of the body and accommodate venous return. The diagnosis is mainly clinical, based on the presence of symptoms including dyspnoea, orthopnoea and fatigue, and signs such as pulmonary and peripheral oedema.
Heart failure is the end result of a number of different pathophysiological processes in which there is injury to the heart with loss or impairment of functioning myocardial cells.5 Compensatory neurohormonal mechanisms are activated in order to maintain adequate cardiac function and tissue perfusion. Activation of the sympathetic nervous system increases heart rate and cardiac contractility, while activation of the renin–angiotensin– aldosterone system increases sodium reabsorption and water retention.
Although these responses are initially beneficial, prolonged overstimulation of the sympathetic nervous system and renin–angiotensin–aldosterone system results in maladaptive cardiovascular remodelling.
The release of natriuretic peptides counteracts the vasoconstricting effects of the sympathetic nervous system and renin–angiotensin–aldosterone system.
Heart failure is often due to myocardial dysfunction and is broadly classified by left ventricular ejection fraction. When the left ventricular ejection fraction is less than 40% it is termed heart failure with reduced ejection fraction. If the ejection fraction is at least 50% the condition is called heart failure with preserved ejection fraction. This accounts for approximately half of all cases of heart failure.6 Although the presentation is clinically indistinguishable from heart failure with reduced ejection fraction, the treatment is different.
Left ventricular ejection fraction in the range 40–49% has recently been termed ‘mid-range’ by the European Society of Cardiology.7 However, given the variation in measuring left ventricular ejection fraction, this is a grey area which requires more research.
Underlying causes of heart failure need to be identified and managed. These include cardiovascular causes such as myocardial ischaemia or infarction, uncontrolled hypertension, valvular disease, atrial fibrillation and tachycardia, and pulmonary embolism. There are also systemic causes, such as infection, thyroid dysfunction, anaemia, poorly controlled diabetes, previous chemotherapy or radiotherapy and peripartum cardiomyopathy. Idiopathic or genetic causes include dilated cardiomyopathy, hypertrophic obstructive cardiomyopathy and arrhythmogenic right ventricular cardiomyopathy. Alcohol and substance abuse, for example amphetamines, can also cause heart failure. Acute triggers causing decompensation may include nonadherence to treatment, iatrogenic factors such as inappropriate drugs, and dietary indiscretions.
Comorbid disease may worsen heart failure or complicate its treatment. Over half of patients with heart failure reported five or more chronic conditions in a US community-based study.8 While cardiac diseases including hypertension, hypercholesterolaemia, ischaemic heart disease and myocardial infarction are the more common comorbidities, chronic obstructive pulmonary disorder, diabetes, depression and renal failure are most strongly associated with adverse outcomes. Renal dysfunction with heart failure, termed cardiorenal syndrome, has a particularly poor prognosis.
Ongoing education about self-management is key to caring for patients with heart failure.9 Use of visual aids can support this education.10
A low-salt diet should be recommended, along with smoking cessation, minimal alcohol intake and regular exercise. A cardiac rehabilitation program11 and a multidisciplinary heart failure team (doctors, nurses, pharmacists)12 have been shown to be beneficial.
Early intervention by the GP to address signs and symptoms of heart failure identified by the patient can reduce hospitalisations for heart failure. An exacerbation of heart failure can be heralded by dyspnoea with usual daily activities, reduced exercise tolerance, abdominal bloating and poor appetite.
Patients should know the weight at which their condition was previously stable. They need to monitor their weight regularly so that they and their caregivers are alert to any weight gain which would suggest fluid retention. The patients need to know what to do when their weight rises above set limits, such as contacting their GP. A fluid restriction for volume overload may be required, with a flexible diuretic regimen if appropriate. Resources are available to help in preparing a heart failure action plan.10
The goal of management of heart failure with reduced ejection fraction is to control symptoms, prevent progression of left ventricular dysfunction, decrease hospitalisation and improve survival. Drugs which block neurohormonal activation are the cornerstone of therapy. They include ACE inhibitors and beta blockers, as well as aldosterone antagonists (Table 1). A new combination of sacubitril and valsartan (a neprilysin inhibitor–angiotensin receptor antagonist) enhances neurohormonal modulation by increasing beneficial natriuretic peptides.
In order to obtain the maximal symptomatic and mortality benefits from these drugs, they should be up-titrated every 2–4 weeks providing that symptoms, heart rate, blood pressure, serum potassium and renal function remain within acceptable ranges (see Fig.).7 Achievement of target doses can take weeks to months (Table 2). Drugs can be up-titrated together in the absence of symptomatic hypotension, however titrating more cautiously one at a time can distinguish which drug is causing an adverse effect. Adverse effects tend to improve over time. If a dose increase is not tolerated, the dose should be reduced and re-titrated once the patient is clinically stable. When significant adverse effects occur, switching to a different drug within the same class should be tried before permanently discontinuing therapy.
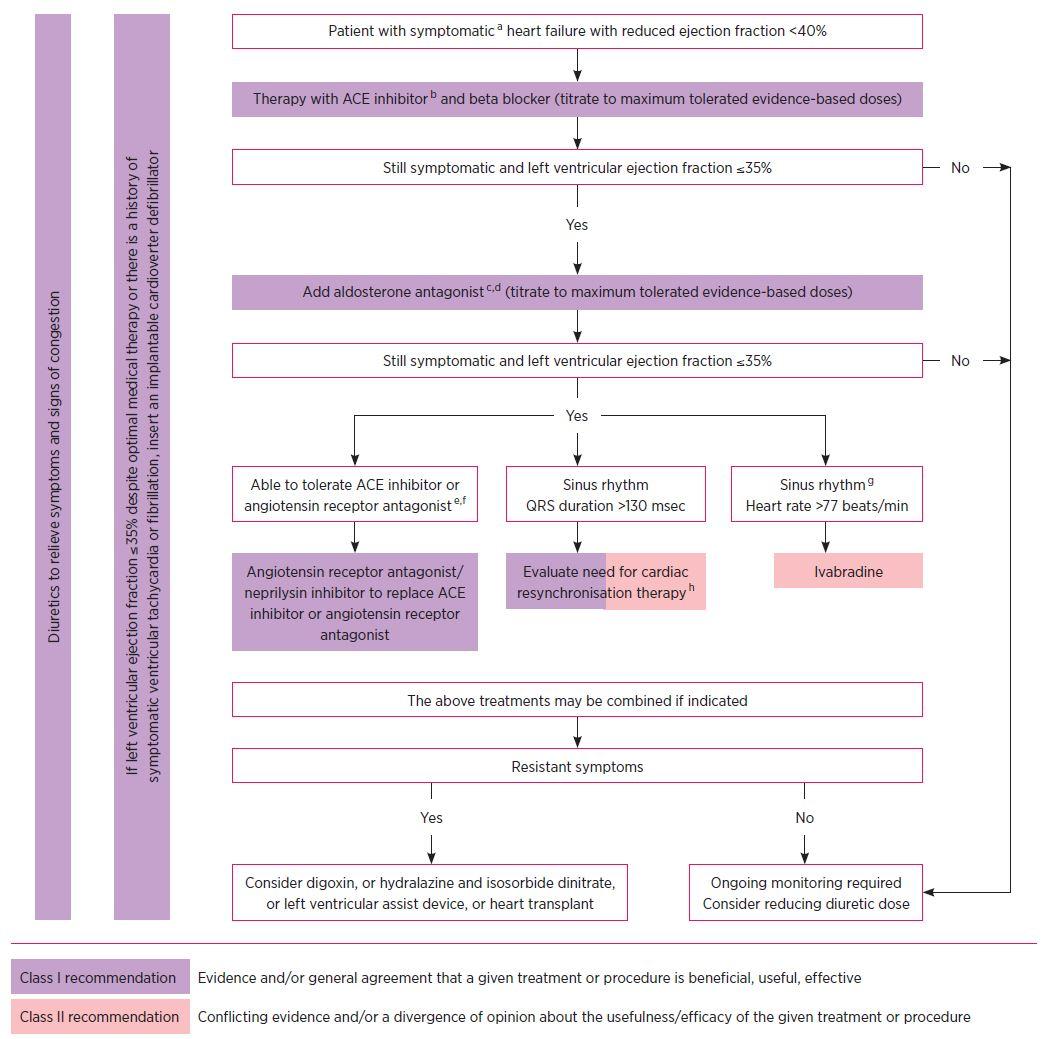
a) New York Heart Association Class II–IV
b) If ACE inhibitor not tolerated or contraindicated, use angiotensin receptor antagonist
c) If aldosterone antagonist not tolerated or contraindicated, use angiotensin receptor antagonist
d) With hospital admission for heart failure in the last six months or with elevated natriuretic peptides
e) With elevated natriuretic peptides
f) In dose equivalent to enalapril 10 mg twice daily
g) With a hospital admission for heart failure in the previous year as per Pharmaceutical Benefits Scheme criteria
h) Cardiac resynchronisation therapy is:
Source: Adapted from Figure 7.1 of reference 7, with permission
ACE inhibitors are first-line therapy in heart failure with reduced ejection fraction and asymptomatic left-ventricular dysfunction. Their use results in a 3.8% absolute reduction (20% relative) in death, with reductions in myocardial infarction and hospitalisation for heart failure.13 Beneficial effects occur early and continue long term, in all age groups. ACE inhibitors reduce the maladaptive effects of chronic renin– angiotensin–aldosterone system activation, including sodium and water retention, vasoconstriction, and cardiac hypertrophy and fibrosis. Studies of angiotensin receptor antagonists (sartans) have not shown a consistent reduction in mortality.14,15 Sartans are therefore considered as a second choice, indicated only in patients intolerant of ACE inhibitors.
Treatment should begin soon after diagnosis, at the lowest dose. Up-titration is recommended if the blood pressure is 90 mmHg systolic or above, and is limited by symptoms rather than the measured blood pressure. If symptomatic hypotension occurs, other vasodilators should be reduced or stopped first and, provided the patient is not congested, diuretics should be reduced or ceased before reducing the ACE inhibitor dose.
A minor worsening of renal function (up to 30% reduction in estimated glomerular filtration rate (eGFR)) is generally acceptable. A small rise in potassium can be expected, but the ACE inhibitor dose should be halved if the potassium concentration exceeds 5.5 mmol/L. If an ACE inhibitor induces a chronic cough, a change to a sartan may be appropriate after other causes of cough have been excluded such as pulmonary oedema or underlying lung disease.
Beta blockers are another important first-line therapy for heart failure with reduced ejection fraction. Given with ACE inhibitors, they are associated with a 4.3% absolute reduction (24% relative reduction) in all-cause mortality and comparable reductions in hospital admissions for patients in sinus rhythm.16 Beta blockers reduce myocardial oxygen demand, protect from ischaemia, have antiarrhythmic effects and reduce sudden cardiac death. Only beta blockers that have been shown to be effective in heart failure should be used. These are bisoprolol,17 carvedilol,18,19 extended-release metoprolol succinate,20 and nebivolol if the patient is over 70 years old (as this drug has only been evaluated in the elderly).21
All patients with heart failure with reduced ejection fraction should be given beta blockers. Start soon after an ACE inhibitor, once the patient is clinically stable and euvolaemic. At first the symptoms of heart failure may worsen so the smallest dose should be used. Aim to titrate up to the target dose or as high as tolerated. Heart rate, blood pressure and symptoms of congestion should be reviewed after each up-titration.
Absolute contraindications to beta blockers include second or third degree atrioventricular block. If these occur, a pacemaker or cardiac resynchronisation therapy should be considered to enable continuation of therapy. Asthma is only a relative contraindication. Chronic obstructive pulmonary disease should be assessed with lung function tests before deciding not to give beta blockers. If there is no significant airway reversibility, the patient should be able to tolerate beta blockers. Usually the impact of beta blocker therapy on lung function tests is minimal and without clinical relevance.22
The dose should be reassessed if clinical deterioration occurs or the heart rate is under 50 beats per minute. As with ACE inhibitors, asymptomatic hypotension does not require a change of therapy. If symptomatic, consider reducing other vasodilators first, or the dose of any diuretic if there is no congestion, before deciding to reduce the dose of beta blocker. Bisoprolol and metoprolol have a less vasodilating effect and may be better tolerated if the blood pressure is borderline, however the additional vasodilating effects of carvedilol may offset the early worsening of heart failure.
Aldosterone antagonists improve survival across the full spectrum of heart failure with reduced ejection fraction. There is an 11% absolute reduction (30% relative) in mortality in severe heart failure,23 a 7.6% absolute reduction (37% relative) in mortality and cardiovascular hospitalisation in mild heart failure,24 and a 2.3% absolute reduction (15% relative) in death in patients with heart failure after myocardial infarction.25 Aldosterone antagonists block the adverse effects of aldosterone activation, which includes sodium and water reabsorption, and cardiovascular fibrosis. These drugs are markedly underused and should be added to ACE inhibitors and beta blockers in all patients who remain symptomatic.
Serious hyperkalaemia can occur, especially with underlying renal impairment. Serum potassium should be closely monitored, at one week and one, two and three months after starting or increasing the dose, then every three months to 12 months, and then four monthly thereafter. The starting dose can be halved if diabetes or renal impairment is present (Table 2). The dose should be halved if potassium exceeds 5.5 mmol/L, and ceased if it is more than 6.0 mmol/L. Gynaecomastia can occur in men, but is less common with eplerenone than with spironolactone.
Sacubitril with valsartan is a new combination which was shown to be superior to enalapril in a large head-to-head trial, with an absolute reduction of cardiovascular death and heart failure hospitalisation of 4.7% (20% relative reduction).26 Sacubitril is a neprilysin inhibitor. It inhibits the degradation of vasoactive peptides including natriuretic peptides, thereby enhancing their beneficial effects such as vasodilation and diuresis. The combination reduces sympathetic tone, aldosterone and myocardial fibrosis and hypertrophy.
Sacubitril with valsartan can replace an ACE inhibitor or sartan if symptoms persist despite optimal medical therapy.7,27 This combination may become first-choice therapy in the future, given its efficacy. However, currently it should be used when a patient has been stabilised on an ACE inhibitor, beta blocker and aldosterone antagonist.
Previous angioedema (due to any cause) is a contraindication. A 36-hour ACE inhibitor washout period is an absolute requirement to reduce the risk of angioedema. The combination lowers the blood pressure more potently and therefore can cause hypotension. This improves over time, but can be addressed by reducing the dose of other vasodilators or halving the starting dose of sacubitril with valsartan.
Other therapies can be added to the essential drugs for heart failure (beta blockers, ACE inhibitors and aldosterone antagonists). They can also be considered secondary choices if the first-line drugs are not tolerated.
Loop diuretics are used by most patients at some stage for symptomatic control of heart failure. They should be used in addition to ACE inhibitors and beta blockers in patients with heart failure with reduced ejection fraction if there is associated symptomatic congestion. Diuretics can often be reduced as doses of neurohormonal blockers are increased.
A small dose of a thiazide or a potassium-sparing diuretic can be added to furosemide (frusemide) or bumetanide for a short period. This has a synergistic diuretic effect for patients with peripheral oedema resistant to treatment with a loop diuretic. Renal function and potassium need to be closely monitored.
A raised resting heart rate is a marker of cardiovascular risk.28 Ivabradine reduces heart rate by inhibiting the sinus node, and results in a 5% absolute reduction (18% relative) in the risk of either cardiovascular mortality or heart failure hospitalisations.29 It is used in heart failure with sinus rhythm when the left ventricular ejection fraction is less than 35% as an add-on to an ACE inhibitor, aldosterone antagonist and maximally tolerated beta blocker if the heart rate is at least 77 beats per minute.29 It can be used if the patient cannot tolerate a beta blocker.
Ivabradine can only be used in sinus rhythm. It does not affect blood pressure, intracardiac conduction or myocardial contractility. It may cause visual symptoms, including flashing lights, which are not associated with retinal damage, and which usually resolve spontaneously. Stop ivabradine if atrial fibrillation develops.
Digoxin is useful for symptomatic control of heart failure in sinus rhythm, but only after therapy with an ACE inhibitor, beta blocker, aldosterone antagonist and diuretic has been optimised. It is a weak positive inotrope and increases vagal tone. In atrial fibrillation digoxin slows the heart rate by reducing atrioventricular nodal conduction.30 Digoxin does not improve survival, but can reduce hospitalisations associated with heart failure and improves symptoms.31 It should be used at a low dose in sinus rhythm, aiming for a serum digoxin of 0.5–0.9 nanogram/mL measured at least six hours after oral dosing.32 Digoxin toxicity may result from deteriorating renal function or dehydration, with symptoms most commonly including nausea, vomiting and drowsiness.33 Digoxin may also be useful for rate control in the treatment of atrial fibrillation in heart failure.
High-dose hydralazine is an arterial vasodilator. Isosorbide dinitrate is predominantly a venodilator. The combination can be used with a beta blocker if the patient is intolerant of ACE inhibitors and sartans. Specialist advice should be sought.
An implantable cardioverter defibrillator should be considered for primary or secondary prevention of ventricular arrhythmias if left ventricular ejection fraction is 35% or less to reduce the risk of sudden death and all-cause mortality.34 This may be implanted alone, or may be combined with cardiac resynchronisation therapy (or biventricular pacing) if the QRS duration on the ECG is prolonged at 130 milliseconds or above with left bundle branch block morphology. This reduces mortality and heart failure hospitalisations and improves symptoms.
Compared to those with a reduced ejection fraction, patients with heart failure with preserved ejection fraction are older, more likely to be female and to have hypertension, atrial fibrillation, diabetes or obesity. The mechanism probably relates to a combination of pathophysiological processes including increased myocardial stiffness, abnormal myocardial relaxation and increased arterial stiffness.
No drug has been shown to improve survival,35 however recent data suggest that in a subset of patients with heart failure and preserved ejection fraction, aldosterone antagonists may improve clinical outcomes.36 Sacubitril with valsartan was found to be beneficial in a phase II study.37 The combination is therefore currently under evaluation for heart failure with preserved ejection fraction.
Diuretics should be used judiciously and over-diuresis avoided. Treatment should focus on aggressive control of concurrent conditions particularly hypertension. Atrial fibrillation should be managed according to guidelines, using a rate control strategy and anticoagulation initially, with a trial of rhythm control for persistent symptoms. Myocardial ischaemia, obesity and anaemia should be addressed. Exercise training can improve quality of life.
Substantial improvements in symptoms are seen after starting drug therapy and often patients will feel back to normal. Left ventricular ejection fraction can sometimes return to normal or close to the normal range. Drugs that confer a survival benefit, in particular ACE inhibitors and beta blockers, should not be stopped, as this may lead to a recurrence of heart failure.38 Diuretics and digoxin (in sinus rhythm) may be reduced and stopped if the patient remains stable.
When the goals of treatment move to palliation and symptom control, ACE inhibitors, beta blockers and aldosterone antagonists should be continued if possible, as they improve symptoms. Down-titration of doses may be needed if hypotension or issues with renal function and electrolytes occur. Statins and digoxin if not being used for atrial fibrillation can be withdrawn. Deactivation of an implantable cardioverter defibrillator should be considered in a patient entering the palliative phase of their illness, or in a patient making an informed end-of-life decision.39 This decision should be undertaken by the patient, their family, GP and specialist.
Many drugs have been shown to exacerbate heart failure.40 Non-steroidal anti-inflammatory drugs (NSAIDs) including COX-2 inhibitors should be avoided as they cause salt and water retention and impair renal function. Non-dihydropyridine calcium channel blockers (verapamil and diltiazem) should be strictly avoided in heart failure with reduced ejection fraction due to their negative inotropic effect. Antiarrhythmic drugs (except beta blockers and amiodarone) and tricyclic antidepressants have pro-arrhythmic potential. Corticosteroids result in salt and water retention. Pioglitazone and some dipeptidyl peptidase 4 (DPP 4) inhibitors may increase the risk of heart failure. Non-potassium sparing diuretics can contribute to digoxin toxicity by causing hypokalaemia, and digoxin concentrations can be increased by amiodarone and spironolactone.
Potential drug–drug interactions occur with various complementary therapies, including St John’s wort, black cohosh and grapefruit juice. These should be avoided.
The type of heart failure determines its treatment. Echocardiography should be used to confirm the underlying aetiology. Patient education is key to successful management.
ACE inhibitors and beta blockers are the cornerstone of therapy for heart failure with reduced ejection fraction. Aldosterone antagonists are added if the patient is still symptomatic. These three drugs reduce mortality and morbidity. Digoxin and diuretics may also be useful if symptoms persist. The combination of valsartan with sacubitril is an evolving alternative to ACE inhibitors in heart failure with reduced ejection fraction. Drug doses need to be titrated to maximally tolerated doses to obtain the most benefit on symptoms and survival.
No drugs have been shown to improve survival in patients who have heart failure with preserved ejection fraction. Treatment should focus on related problems such as hypertension.
Conflict of interest: none declared

Clinical pharmacologist and heart failure specialist physician, Alfred Health, Melbourne
Heart failure clinical nurse specialist, Alfred Health, Melbourne


