Article
Drugs in secondary stroke prevention
- Chris Tremonti, Mark Thieben
- Aust Prescr 2021;44:85-90
- 1 June 2021
- DOI: 10.18773/austprescr.2021.018
After an ischaemic stroke or transient ischaemic attack, patients have a high risk of having another stroke. Secondary stroke prevention includes antiplatelet therapy, statins and antihypertensives.
Aspirin, clopidogrel, or a combination of aspirin with dipyridamole are first-line options for secondary stroke prevention in the absence of atrial fibrillation.
Dual antiplatelet therapy has a benefit in the first three weeks after stroke, but patients should change to a single antiplatelet drug after this time.
Anticoagulants are indicated if the patient has atrial fibrillation. Avoid combinations of anticoagulants and antiplatelet drugs.
Patients should be started on statins after an ischaemic stroke. High doses are recommended even if cholesterol concentrations are normal.
Antihypertensive drugs are recommended for all patients with systolic blood pressures greater than 140/90 mmHg. ACE inhibitors, calcium channel blockers and diuretics are first-line options.
Each year almost 20,000 Australians have a stroke, the majority of which are ischaemic.1 The 10-year recurrence rate following a first stroke is over 40%.2 To prevent recurrences patients are managed with a combination of drugs and lifestyle modification. Pharmacotherapy is critical for optimising outcomes for patients after an ischaemic stroke or transient ischaemic attack (see Fig.). Treatment recommendations change regularly, and as such there are a set of living guidelines for secondary stroke prevention that are continually reviewed and updated.3 Adherence to treatment is also important.
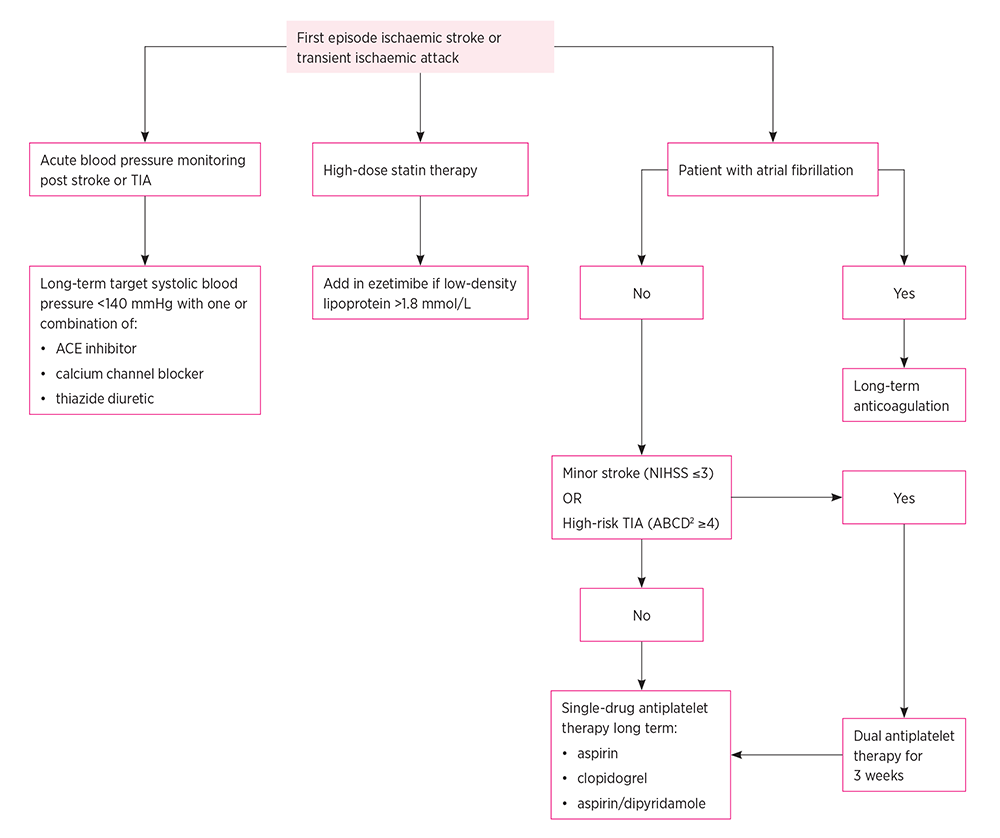
NIHSS National Institutes of Health Stroke Scale
The efficacy of antiplatelet drugs for secondary stroke prevention is well established.4 Antiplatelet therapy should start as soon as possible following a stroke or transient ischaemic attack.5 Current Australian guidelines recommend either aspirin, clopidogrel or a combination of aspirin and dipyridamole (see Table). Antiplatelets carry some risk of gastrointestinal bleeding. The routine use of proton pump inhibitors is restricted to those considered higher risk, for example patients with a history of gastrointestinal ulcer, or those over 60 years with gastro-oesophageal reflux disease.6
Table - Comparative efficacy of antiplatelet drugs for secondary stroke prevention
|
Aspirin versus placebo |
Clopidogrel versus placebo |
Aspirin/dipyridamole versus placebo |
|
|
Recurrent stroke (up to 27 months) |
Odds ratio 0.78 (95% CI 0.63–0.99) |
Odds ratio 0.68 (95% CI 0.53-0.92) |
Odds ratio 0.69 (95% CI 0.56-0.89) |
|
Bleeding (up to 27 months) |
Odds ratio 2.33 (95% CI 1.73–3.30) |
Odds ratio 1.79 (95% CI 1.23-2.78) |
Odds ratio 1.95 (95% CI 1.43-2.78) |
|
Serious vascular event (up to 27 months) |
Odds ratio 0.83 (95% CI 0.71-0.96) |
Odds ratio 0.74 (95% CI 0.65-0.86) |
Odds ratio 0.72 (95% CI 0.63-0.83) |
Adapted from reference 3
CI confidence interval
A 2016 meta-analysis found that aspirin at daily doses of 75–162 mg or 500–1500 mg reduced long-term recurrence of stroke more than placebo.7 However, there was an increased risk of bleeding with the increased dose range, so typically doses of 75–150 mg are used. The benefit of aspirin has been shown to be even more marked for secondary stroke prevention in the first six weeks post stroke.5
Dipyridamole should not be used alone in stroke prevention. In trials it was combined with aspirin, typically as aspirin 25 mg and dipyridamole 200 mg. This is an acceptable antiplatelet combination for patients with non-cardioembolic ischaemic stroke or transient ischaemic attack.
The 2006 ESPRIT trial found that the combination of aspirin and dipyridamole had a benefit over aspirin alone with regard to secondary stroke risk, and non-fatal bleeding.8 It is worth noting however that the majority of patients were randomised after more than one month, and so it is unclear if aspirin/dipyridamole has benefit over aspirin immediately after a stroke.
Dipyridamole has a vasodilatory action and headache is a common adverse effect which may lower adherence to treatment.9 Dipyridamole’s vasodilatory effect also means care should be used in patients with unstable angina or aortic stenosis.
Clopidogrel, a P2Y12 inhibitor, has efficacy for secondary stroke prevention at doses of 75 mg.10 A 2019 meta-analysis found a benefit for clopidogrel over aspirin and aspirin/dipyridamole for reducing major bleeding and intracranial haemorrhage.11
Ticagrelor, another P2Y12 antagonist, has not been shown to offer a benefit over aspirin for monotherapy.12 It is not recommended in guidelines or approved by the Therapeutic Goods Administration for stroke prevention in Australia.
Patients may have ‘breakthrough’ cryptogenic strokes despite antiplatelet therapy. It is worth discussing the patient’s adherence to treatment and working with them on strategies to improve this if there is a problem.13
Studies have shown that patients adherent with aspirin benefit from a change to a different antiplatelet drug if they have a breakthrough ischaemic stroke.14,15 ‘Clopidogrel resistance’ is a phenomenon well studied in acute coronary syndrome, but less so in stroke, making it a challenge to guide management of breakthrough stroke on clopidogrel.16 Screening for clopidogrel resistance is not currently recommended.17
Dual antiplatelet therapy in secondary stroke prevention has received increased attention due to two major randomised controlled trials – CHANCE and POINT. CHANCE found aspirin and clopidogrel given together for the first 21 days after a high-risk transient ischaemic attack (ABCD2 ≥4)18 or minor stroke (National Institutes of Health Stroke Scale ≤3)19 reduced recurrence without a risk of increased bleeding compared to aspirin alone.20 The POINT study showed a reduction in ischaemic stroke at 90 days for patients on the aspirin/clopidogrel combination compared to aspirin alone in minor stroke or high-risk transient ischaemic attack, at the cost of an increased rate of major haemorrhage.21 A subsequent meta-analysis including both trials has suggested that dual antiplatelets appear to be most beneficial in the first three weeks following minor stroke.22 In Australia, the Stroke Foundation currently advises using dual antiplatelet therapy for three weeks after a non-valvular, non-arrhythmic, minor ischaemic stroke or high-risk transient ischaemic attack then switching to monotherapy.3 There is no evidence to continue dual therapy beyond 90 days. For larger strokes (NIHSS >3), the risk of bleeding from dual antiplatelet therapy outweighs the benefits and is not routine practice.
The combination of aspirin with ticagrelor was recently compared to aspirin alone in the first 30 days after a stroke. This THALES study found the combination to be superior for prevention of stroke or death, but with an increased risk of major bleeding.23 Ticagrelor is not currently listed on the Pharmaceutical Benefits Scheme for stroke prevention, and like other combinations, the combination with aspirin has no evidence beyond 30 days.
Dual antiplatelet therapy will typically be used for 30 days after carotid artery stenting. However, there is no evidence to support dual antiplatelet therapy after carotid endarterectomy.24
The evidence for anticoagulants for the secondary prevention of ischaemic stroke in a patient with non-rheumatic atrial fibrillation without mechanical heart valves is unequivocal.25,26 The direct oral anticoagulants are now preferred to warfarin for secondary stroke prevention. This is because a meta-analysis found non-inferiority for preventing ischaemic stroke and superiority for rates of haemorrhagic stroke.27 Warfarin does have some advantages in the risk of gastrointestinal bleeding, and can also be used in patients with an estimated glomerular filtration rate (eGFR) below 15 mL/minute. The choice of direct oral anticoagulant is individualised based on renal function, ability to adhere to the dosing schedule and the likely need for reversal of anticoagulation.28
There are concerns that cryptogenic strokes may be due to undiagnosed paroxysmal atrial fibrillation,29,30 creating the idea that anticoagulants may have a role even if the arrhythmia is not detected.31,32 However, evidence to support this is lacking, and anticoagulants post stroke without evidence of atrial fibrillation are not recommended for secondary stroke prevention due to the increased risk of bleeding.33
There is no role for antiplatelets in secondary stroke prevention in patients with atrial fibrillation as they should be anticoagulated. After a stroke, patients taking anticoagulants for atrial fibrillation should stop antiplatelet drugs, unless there is another indication for antiplatelet therapy, such as previous acute myocardial infarction or coronary stents. Clinicians should liaise with the patient’s cardiologist with a view to stopping the antiplatelet drugs when possible.
The Australian Clinical Guidelines for Stroke Management currently recommend a reduction of systolic blood pressure to less than 140 mmHg.3 A target of below 130 mmHg has been suggested to offer a small additional benefit in secondary stroke prevention for patients with lacunar infarcts. This comes at the risk of increased unsteadiness, especially in older patients.34,35 The blood pressure target will also depend on evidence of other sequelae of hypertension, such as renal impairment.
ACE inhibitors, calcium channel blockers and thiazide diuretics are first-line options for blood pressure control after a stroke.36 The choice should be individualised for each patient. A large meta-analysis of cardiovascular outcomes found beta blockers may be inferior to other antihypertensive drugs in stroke prevention.37
Adherence to diuretics has been shown repeatedly to be worse than with other antihypertensives.38 The adherence to the other drugs is around 80% one year after the stroke. Programs designed to increase patient adherence and improve blood pressure long term have shown some benefit on adherence, but not on blood pressure.39 Of concern, however, is evidence that people who remain hypertensive after a stroke are under-prescribed antihypertensive drugs despite a clear benefit in stroke prevention.40
High-dose statins, such as atorvastatin 80 mg or rosuvastatin 40 mg, are first-line treatment for all patients following ischaemic strokes regardless of their cholesterol.3 This is because a meta-analysis found high-dose statins offered a protective effect against further ischaemic strokes even when cholesterol was not elevated.41 There had been concerns that statins may cause an increase in intracerebral haemorrhage based on results from the SPARCL trial and the Heart Protection Study.42,43 However, this was not borne out in a subsequent meta-analysis, which also reported that statins improved all-cause mortality, functional outcome, and the risk of stroke regardless of type.44 In patients who cannot tolerate high-dose statins, low-dose statins should still be tried.
A 2020 randomised controlled trial found that a target low-density lipoprotein concentration of less than 1.8 mmol/L had benefit in protecting patients post stroke from cardiovascular events, compared to a target of 2.3–2.8 mmol/L.45 Patients in the lower target group typically received ezetimibe if their cholesterol remained elevated, although there was no fixed regimen. Ezetimibe is also recommended for patients who are statin intolerant as second-line therapy.46 This is mainly based on the IMPROVE-IT trial, which studied patients with acute coronary syndrome.47 It is unclear if ezetimibe works as monotherapy.48 The main adverse effects of ezetimibe include myalgias, headaches and hepatitis.
Fibrates have not been shown to be beneficial in secondary stroke prevention. They are not recommended in treatment guidelines.49,50
After a stroke, patients are at risk of further ischaemic strokes, particularly in the first few weeks. Antiplatelet drugs, statins and antihypertensive drugs are the mainstay of pharmacotherapy for secondary stroke prevention. If dual antiplatelet therapy is used after a stroke, clinicians should ensure patients return to single drug therapy three weeks later. Patients with atrial fibrillation should be anticoagulated. Combinations of anticoagulants and antiplatelets should be avoided if possible. Liaise with the patient’s neurologist and cardiologist if the patient is taking anticoagulants and antiplatelets to confirm whether combined treatment is intended.
The target blood pressure should be less than 140 mmHg systolic. ACE inhibitors, calcium channel blockers or thiazide diuretics can be used. Statins are first-line treatment and a target low-density lipoprotein of less than 1.8 mmol/L is now recommended.
Conflicts of interest: none declared
Australian Prescriber welcomes Feedback.
Advanced trainee in Clinical Pharmacology, Royal Prince Alfred Hospital
Neurologist, Royal North Shore Hospital Sydney


