Article
Good nutrition for good surgery: clinical and quality of life outcomes
- Lynne Daniels
- Aust Prescr 2003;26:136-40
- 1 December 2003
- DOI: 10.18773/austprescr.2003.100
Undernutrition is common in patients admitted for surgery and is often unrecognised, untreated and worsens in hospital. The complex synergistic relationship between nutritional status and the physiological responses to surgery puts patients at high nutritional risk. There are clear prospective associations between inadequate nutritional status and the risk of poorer outcomes for surgical patients, including infection, complications and length of stay. However, practically and ethically evidence that nutritional interventions can significantly reduce these poor outcomes is difficult to obtain. Nevertheless health professionals have a duty of care to ensure our patients are properly fed, by whatever means, to meet their physiological requirements.
Well-nourished patients respond to, and recover from illness and surgery better than undernourished patients. While overnutrition is widely thought to be the primary nutritional problem in Australia, undernutrition and/or malnutrition are prevalent in population sub-groups. Studies consistently show that 30–40% of patients show evidence of poor nutrition on admission to hospital and that both normal and sub-optimal nutritional status deteriorate in hospital.1The physiological and psychosocial stresses of surgery increase the risk of poor nutritional status, which is clearly linked to poorer outcomes.2,3Poor nutrition therefore has clinical, financial and quality of life consequences.3
Adequate nutritional status is more than the absence of nutrient deficiency disease. It is a broad concept which infers that an individual can achieve a food intake sufficient to meet their requirements for specific nutrients to support optimal health and well-being.
There is no universally accepted definition of malnutrition. The term is widely associated with severe food deprivation and the classic consequences of kwashiorkor, marasmus or micronutrient deficiency. Malnutrition may refer to overnutrition, but more commonly is used interchangeably with undernutrition.
Undernutrition refers to a continuum of inadequate nutritional status. It extends from inadequate intake and increased risk of poorer health outcomes, through to measurable functional or clinical changes that influence outcomes and are potentially reversed by nutritional interventions, and finally to clear physical and biochemical evidence of protein, energy or micronutrient deficiency.
There is no ‘gold standard’ for identifying either nutritional risk or nutritional status. Nutrition screening aims to identify factors associated with poor nutrition and hence individuals at nutritional risk. It needs to be valid, simple, easy to interpret and sensitive so that it can be widely and consistently implemented by non-specialists. A range of screening tools have been developed and variably validated.4They include self-reported indicators of either risk or direct evidence of poor or reduced intake (Table 1).
Table 1 - Nutrition screening and assessment – commonly used indicators
|
Nutritional screening identifies patients ‘at risk’ |
|
|
Subjective/self-reported
|
Objective
|
|
Nutritional assessment assesses the nutritional status of patients identified as ‘at risk’ |
|
|
|
If screening identifies individuals at risk, they should be referred for detailed assessment of their nutrition. Nutritional assessment is a comprehensive process used to define the patient's nutritional status rather than risk. It helps to quantify the risk of complications and can be used to plan and monitor nutritional support4(Table 1).
Limitations of screening and assessment include reliance on self-reported data, inaccurate measurement of stature in injured or elderly patients and confounding of serum protein concentrations by infection and trauma. Nevertheless, the risk factors in Table 1 should be routinely considered in assessment and follow-up of pre- and postoperative patients. The general consensus is that unintentional weight loss, regardless of initial weight, is the simplest and most reliable way to identify nutritional risk2,4(see Box 1).
Special attention should be paid to those patients whose disease status and symptoms incur particular risk of either compromised intake and/or increased requirements. Self-reported weight and height are unreliable so regular monitoring and documentation of weight becomes critical. Use of triceps skinfold (TSF) and mid-arm muscle circumference (MAMC) should be considered in patients with ascites or fluid retention (Table 1).
Reliable and valid measurements of triceps skinfold and mid-arm circumference are relatively difficult and training is needed. Reference percentile data are available5,6but care should be taken to ensure the reference group is relevant to the individual patient.
Self-reported unintentional weight loss, being underweight on admission, and a decline in nutritional status during admission, have all been associated with poor outcomes.3A 1994 study reported that 40% of 500 patients sequentially admitted across five sub-specialities (including general and orthopaedic surgery) were at least mildly undernourished (body mass index < 20, TSF or MAMC < 15th percentile).1Notably, only 34% of the patients were overweight. Nutritional information was documented for only 48% of the undernourished patients. Of the 112 patients in hospital for approximately seven days, 64%had lost 5-10% of their body weight when they were discharged. At discharge, 75% of the patients who were undernourished on admission had lost weight and only 13% had gained weight. There are a range of structural and practical issues that contribute to the exacerbation or development of undernutrition in hospitals (see Box 2).
There have been few prospective studies of the prevalence and outcomes of documented weight loss before admission. A study of 221 surgical patients showed objective weight loss during the month before admission in 26% (mean loss 6%) with 10% losing more than 5% of their weight (mean loss 10%), which was associated with increased length of hospital stay.4
The role of the general practitioner
The prevalence of undernutrition on admission means that this problem and the attendant implications for health and well-being must exist in the community. If general practitioners are alert to the possibility they may be able to prevent or ameliorate undernutrition before admission or at least warn the hospital that the patient may be undernourished.7
Pre- and post-surgery it is necessary that general practitioners closely monitor weight and the self-reported screening indicators outlined in Table 1. Where appropriate it is important to encourage and highlight the need for a high-energy intake. It may be helpful to recommend use of oral nutritional supplements, although these are expensive and compliance is often poor. Referral to a dietitian for ongoing monitoring and management should be considered for patients at particular risk (e.g. dysphagia, gastrointestinal problems) and those who are substantially underweight or consistently losing weight.
The complex response to the physiological stress of surgery and injury, mediated via hormonal changes and the sympathetic nervous system, is one of hypermetabolism and catabolism.2There is marked salt and water retention and increases in basal metabolic rate and hepatic glucose production. Wound healing accounts for 80% of the increased glucose production and also requires protein synthesis.2Fat (adipose tissue) and protein stores (lean muscle mass) are mobilised to meet the needs of glucose and protein synthesis which results in negative nitrogen balance and weight loss. Overall, the catabolic response increases energy and protein requirements, the magnitude and duration depending on the extent of the surgery.2A critical point is that semi-starvation (that is, intake consistently below potentially increased requirements) is also catabolic and further exacerbates negative nitrogen balance and weight loss. Indeed, recent evidence suggests the catabolic response to surgery may not be obligatory and can be prevented by adequate intake.2,3
Adequate energy and protein intakes are essential to limit net protein and fat losses. However, many patients are unable to eat enough to meet increased needs and/or prevent losses after surgery. Common and often underrated issues such as pain, nausea, medication, dry mouth, gastric discomfort and distension, fasting, unpleasant procedures, anxiety, unfamiliar food and hospital routines all potentially reduce appetite and intake. Inadequately or unfed patients will rapidly deplete their reserves of protein and fat. This has significant clinical consequences, particularly for those with preoperative undernutrition.
Positive outcomes for surgery depend heavily on adequate immune defence and wound healing. Both rely on enhanced synthesis of new proteins, which is significantly limited by negative nitrogen and energy balance. A key point is that positive nitrogen balance (net protein synthesis) cannot be achieved with negative energy balance. Semi-starvation will result within days rather than weeks, when intake fails to meet requirements, particularly for protein and energy.
The consequences of significant semi-starvation in healthy persons are summarised in Table 2. These problems are also common after surgery, so it is likely that the undernutrition associated with the surgery is contributing to poor outcomes for surgical patients (Table 2).
Table 2 Outcomes associated with semi-starvation and undernutrition in healthy people and surgical patients
|
Semi-starvation – healthy people and surgical patients8 |
|
|
|
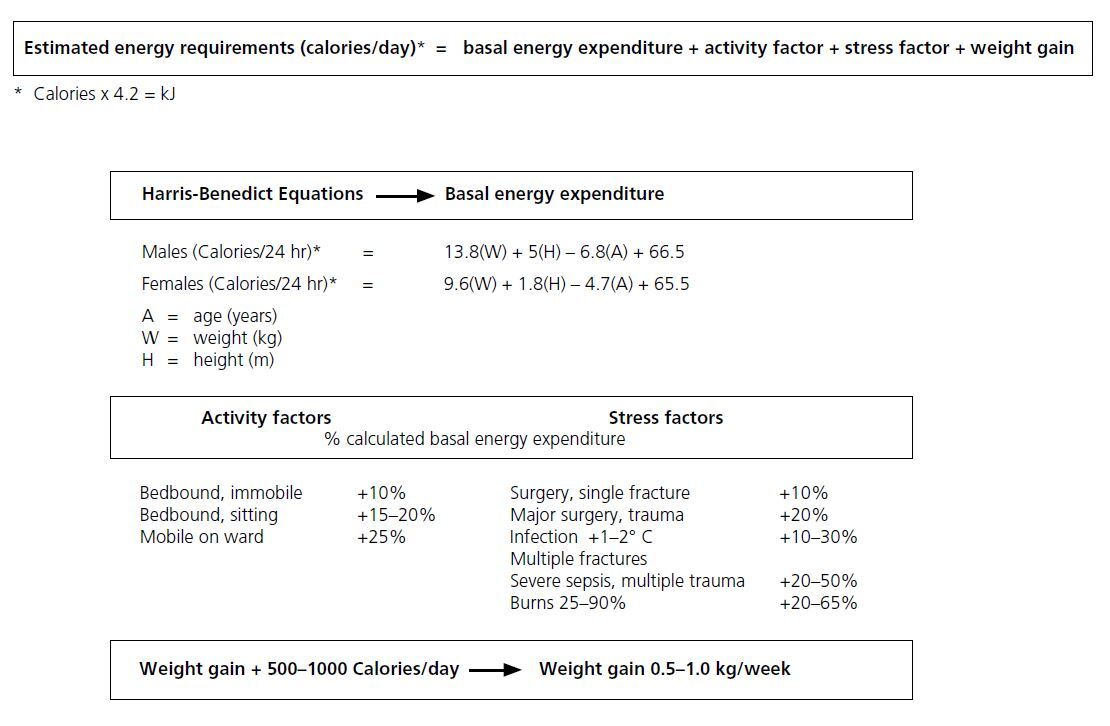
Nutritional interventions can only be effective if energy requirements are both accurately estimated and then achieved. The standard approach is to estimate energy requirements from basal energy expenditure, using regression equations and activity and stress factors (see table 3). Energy requirements range from 85–150 kJ/kg. Protein requirements are usually set at 7–8% of energy needs, although severely ill or injured patients may require 15–20% of their energy as protein. This is approximately 1.5–2.0 g of protein/kg of body weight.2Further research is required to characterise specific amino acid and micronutrient requirements in surgical patients.3
Table 3 - Estimation of basal energy expenditure and total energy requirements 9
Ongoing monitoring is needed to evaluate the accuracy of the patient's estimated requirements. This also ensures that the patient is receiving the prescribed level of nutrition support to meet these requirements.
The indications, options and limitations of nutritional support are summarised in table 4. The golden rule is ‘if the gut works, use it’. There is little evidence that parenteral is more effective than enteral nutrition, but it is certainly costlier and associated with higher risks of serious complications, particularly infection.3,8There is evidence that early (within 24 hours) enteral feeding has significant benefits over late enteral and parenteral feeding.2,3Prolonged absence of nutrients from the gut alters gut flora and may compromise amino acid metabolism. It also changes and reduces mucosal structure and function.2
Table 4 - Indicators for, modes of delivery, limitations and monitoring of nutrition support for surgical patients
|
Patients needing nutritional support |
|
||||||
|
Oral
|
Enteral
|
Parenteral
|
|||||
|
DELIVERY |
Food fortification
|
Oral supplements
|
Nasogastric
|
Nasoenteral
|
Gastrostomy/(jejunostomy)
|
Peripheral
| Total parenteral nutrition
|
LIMITATIONS |
|
|
|
|
|
|
|
|
MONITOR |
|
|
|
||||
There is a wide range of proprietary oral and enteral polymeric (intact macronutrients) feeding products that are isotonic and nutritionally balanced. If energy intake is adequate, these products will meet the requirements for macro- and micronutrients. They are lactose free and usually provide 1.0 Cal/mL (4.2 kJ/mL). There are also more nutrient dense, higher osmolality formulae (1.5 and 2.0 Cal/mL).
Overall, there are few differences between the formulae that result in demonstrable clinical advantage although there is some variation in the quantity and type of fibre and fatty acids. The hyperosmolar, hydrolysed, elemental feeds are intended for patients with impaired digestion and there are condition specific feeds, for example for liver or renal failure, critical care, or pulmonary disease. These formulae are expensive and there is insufficient independent evidence of clinical advantage.9
Routes of feeding should be considered as complementary not competitive. The central issue is that nutrient requirements are met and withdrawal of enteral or parenteral support should be gradual in response to clear evidence that the individual is able to consistently meet the deficit in energy intake by the oral route. Commonly, tubes and lines are removed after a day or two of very limited oral intake in the belief (or hope) that the patient has started eating. In reality, it may take days or weeks for oral intake to fully meet requirements and meanwhile the advantages of the early nutritional support are eroded.
Two recent studies10,11present evidence for the effectiveness of oral supplements in surgical patients. Patients with only marginal undernutrition and not needing enteral or parenteral nutrition were randomised post-gastrointestinal surgery to oral supplements (n = 43) or usual ward diet (n = 43). These supplements contained 6.3 kJ/mL and 0.05 or 0.06 g protein/mL. The treatment group lost less weight (2.2 versus 4.2 kg (p < 0.001)), had fewer complications (n = 4 versus 12, p < 0.05) and felt less fatigued.10A 10-week study11showed that malnourished postoperative patients who received oral supplements (n = 52) lost less weight and showed improved quality of life and lower antibiotic use than controls (n = 49) randomised to receive a normal diet.
There is good evidence that undernutrition, particularly in surgical patients, is prospectively associated with increased risk of poor outcomes.2,3,8,10,11However, there is not a clear cause and effect relationship and it is very difficult to isolate the confounding effect of the disease process. There is a paucity of ‘gold standard’ evidence that nutrition support will reverse poor outcomes. Well-designed prospective randomised controlled trials are rare and exceedingly difficult to implement (table 5). A key issue is that in many studies too little nutrition support is given for too short a time and potential effects may be diluted. Absence of quality evidence is not the same as evidence of absence of effect.
Table 5 - Ethical and practical limitations in the design and implementation of randomised controlled trials to establish effectiveness of nutrition interventions
|
need large numbers of patients and multicentre trials to provide sufficient power |
effect most likely to be seen in undernourished |
individual requirements may not be met and effect diluted |
|
• aetiology of undernutrition is complex and multifactorial • patient groups extremely heterogeneous • clinical course and severity of disease/surgery are major confounders • variation in treatment/procedures between study sites |
• although under ‘usual care’ many cases unrecognised and untreated, once identified cannot withhold intervention • placebo enteral/parenteral feeding unethical • blinding impossible • consent to ‘no treatment’ difficult |
current methods of estimation of energy requirements will theoretically underestimate need for 50% of individuals • need to individualise nutrition support prescription adds complexity • too little nutrition support given for too short a period of time • compliance with oral supplements notoriously poor, volumes frequently inadequate, delivery unreliable • prescribed enteral intakes often not met, feeding frequently interrupted |
|
outcomes rarely include quality of life trials very expensive, funding most likely from companies marketing formulae, therefore independence of data could be questioned |
||
The clinical and financial outcomes of undernutrition are frequently unrecognised, underrated and unacknowledged in surgical and other groups of hospital patients. Much undernutrition remains undiagnosed and untreated, despite the existence of tools to identify the problem and availability of nutritional support. Factors contributing to undernutrition in hospital patients include lack of awareness, inadequate nutrition knowledge and training of staff, limited availability of multidisciplinary specialist clinical nutrition teams and services, and lack of policies, procedures, guidelines and standards of care.9Large, well-designed studies are required to find out if nutritional interventions are independently effective, but given the ethical and practical problems, these studies may not be carried out. However, we have a duty of care to ensure our patients are properly fed, by whatever means, to meet their physiological requirements. Hospitals should review their systems to assess patients’ nutritional needs and ensure these are met.
The following statements are either true or false.
1. Postoperative patients' basal energy requirements reduce while they are immobile in bed.
2. Poor dentition is a risk factor for undernutrition.
Answers to self-help questions
1. False
2. True
