Article
High-risk medication alert: intravenous potassium chloride
- James F. Reeve, Yvonne M. Allinson
- Aust Prescr 2005;28:14-6
- 1 February 2005
- DOI: 10.18773/austprescr.2005.010
Patients have died in hospitals both in Australia and overseas after being mistakenly injected with potassium chloride instead of normal saline. In an effort to reduce the risks associated with the use of intravenous potassium chloride, the Australian Council for Safety and Quality in Health Care has issued a high-risk medication alert for intravenous potassium chloride. This alert contains recommendations for prescribing, storage, preparation and administration of intravenous potassium chloride.
An elderly patient was admitted to hospital for investigation of weight loss and anaemia. The patient had a history of chronic renal failure and hypertension with underlying coronary disease. X-rays disclosed deteriorating cardiac failure.
As part of the investigation a colonoscopy was performed, but a perforation occurred necessitating a sigmoid colectomy. In the intensive care unit the patient developed cardiac complications with rapid atrial fibrillation and hypotension. The potassium concentration was 3.6 mmol/L (normal range 3.5–5.0 mmol/L) and was suspected as the cause of the atrial fibrillation. A dose of 2 g of potassium chloride was prescribed. This was administered as an intravenous infusion over a period of less than 10 minutes. The patient suffered a cardiac arrest and died. The inquest found that the rapid infusion of potassium chloride caused the cardiac arrest, which led to the death of the patient.1
An elderly patient was admitted to hospital for terminal care. The patient was receiving total parenteral nutrition via a Hickman (Cook) intravenous catheter. This was flushed with heparinised saline three times per week. Instead of saline, two ampoules of potassium chloride were inadvertently selected and used to flush the catheter. Before the flushing was completed, a nurse observed that the patient 'clutched her chest and rolled her eyes'. The patient immediately had a cardiac arrest and died.
The coroner's investigation found that routine procedures for checking of the correct drug against the medication chart were not followed.1
The risks associated with intravenous potassium chloride are well known. If it is injected too rapidly or in too high a dose, it may cause cardiac arrest within minutes. The effect of hyperkalaemia on the heart is complex – virtually any arrhythmia may be observed.2
The true incidence of potassium-related fatalities and incidents is unknown. Fatal intravenous injection of potassium produces no specific anatomic changes and subtle, if any, findings at autopsy.3 A search of the national Australian database of coronial findings (the National Coroners Information System) containing data from all States and Territories from January 2001 found no fatalities associated with potassium chloride. A more detailed keyword search was possible within the Victorian case management system. This uncovered five fatalities associated with potassium chloride between 1992 and 1997 and an open case from July 2003. The Australian Incident Monitoring System (AIMS) and AIMS Anaesthetic databases contain details of more than 30 intravenous potassium chloride-related incidents (no fatalities).4
Medication incidents associated with intravenous potassium chloride tend to occur due to inadvertent selection and administration of an ampoule of potassium chloride in place of another drug with similar appearance (Fig. 1), or due to an error in preparation or administration.
Fig. 1 | |
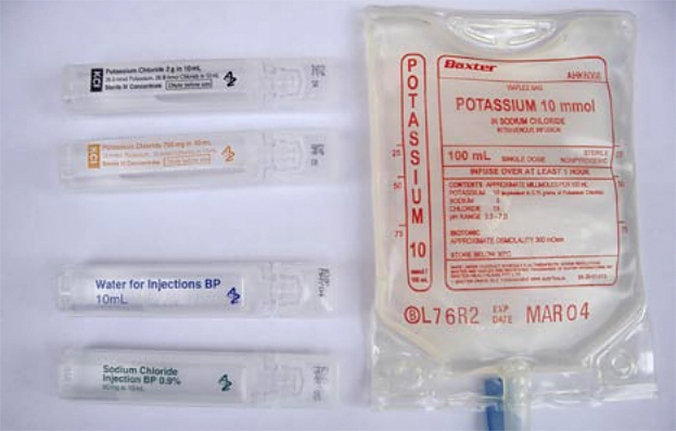 | |
On left, 10 mL ampoules containing, from the top:
|
On right:
|
Analysis of incidents associated with intravenous potassium chloride have led patient safety organisations in the USA, Canada, the UK and Australia to recommend a simple way to prevent these tragic deaths - 'replace concentrated ampoules with large-volume premixed solutions in general ward areas in acute care facilities'.4
In areas where ampoules of concentrated solution need to be retained, it is recommended that they are stored separately and are readily identifiable from preparations with similar packaging. Overseas and in Australia, manufacturers are taking steps to reduce the problem by colour-coding and/or changing the shape of potassium chloride ampoules.
The Australian Council for Safety and Quality in Health Care has issued a high-risk medication alert for intravenous potassium chloride (see box for recommendations).5 The alert covers prescribing, storage, preparation and administration of intravenous potassium chloride. The alert, and tools to action the recommendations in the alert, is available at www.safetyandquality.org
| Recommendations from Safety and Quality Council medication alert: intravenous potassium chloride can be fatal if given inappropriately5
|
|
1. REMOVE AMPOULES OF POTASSIUM CHLORIDE FROM WARD STOCK AND REPLACE WITH PREMIXED SOLUTIONS. Due to the risk associated with intravenous potassium chloride, ampoules of potassium chloride SHOULD NOT be kept as a stock item in wards. 2. In critical areas where high concentrations and doses of potassium chloride are necessary, do a risk assessment to determine whether it is appropriate to keep the ampoules as a stock item and develop a protocol for safe preparation and use. 3. Assess the storage of potassium chloride ampoules and premixed solutions to ensure they are stored separately and are readily identifiable from preparations with similar packaging. The recommendations also apply to ampoules of potassium phosphate or other concentrated potassium salts. |
Project Pharmacist, Project Pharmacist
Executive Director, The Society of Hospital Pharmacists of Australia; and Adele Stevens, Assistant Director (retired), Management Group, Australian Council for Safety and Quality in Health Care
