Article
How to adjust drug doses in chronic kidney disease
- Maurizio Stefani, Richard F Singer, Darren M Roberts
- Aust Prescr 2019;42:163–7
- 1 October 2019
- DOI: 10.18773/austprescr.2019.054
Drugs excreted by the kidney require dose reduction in chronic kidney disease. This adjustment depends on the severity of the disease and what proportion of the drug is eliminated by the kidneys.
The estimated glomerular filtration rate can generally be used to guide dose adjustment in patients with stable kidney function. However, the formula can be misleading in some patient subsets and other approaches are required.
At extremes of body mass, the estimated glomerular filtration rate can under- or overestimate kidney function. It may need to be adjusted for body surface area, particularly for drugs with a narrow therapeutic range or requiring a minimum concentration to be effective. Close monitoring of drug effect and toxicity is also needed and can be supported by therapeutic drug monitoring.
For short courses of drugs with a wide therapeutic index, dose adjustment may not be needed.
Alternative methods for quantifying kidney function include the Cockcroft-Gault formula (estimates creatinine clearance) or direct measures of glomerular filtration rate using exogenous isotope compounds. These are not commonly required.
Chronic kidney disease is defined by a glomerular filtration rate (GFR) of less than 60 mL/min/1.73 m2 or evidence of glomerular-tubular injury, for example haematuria or proteinuria. The diagnosis is becoming more common with 1.0% of Australians being diagnosed in 2017–18. In those over 75 years old, the prevalence was 4.6%.1 However, biochemical results indicate the actual prevalence may be closer to 10% in adults,2 and more than 30% in a hospital population.3
Many drugs are eliminated by the kidney to some extent. If the dosage is not appropriately decreased in a patient with chronic kidney disease, drug concentrations can increase, risking adverse drug reactions. On the other hand, unnecessary decreases in dosage may result in undertreatment, or changing to an alternate drug with a narrower therapeutic index, lower efficacy or both. Examples include changing a patient with chronic kidney disease from metformin to a sulfonylurea (lower effectiveness and reduced long-term benefit), or rivaroxaban to warfarin (narrower therapeutic index and requiring more blood tests).
The requirement for dose adjustments in adults with chronic kidney disease should be anticipated at the point of prescribing. It is important for prescribers to understand that there are different methods of calculating the dose adjustments in these patients.
The need for and extent of dose adjustment depends on the severity of chronic kidney disease, the proportion of the drug eliminated by the kidney, the risk of adverse effects from the drug, the duration of treatment and if the drug has active or toxic metabolites that rely on the kidney for elimination.4 Drug toxicity due to an inappropriately high dosage is seen after multiple doses due to drug accumulation, rather than after the first dose.5 The dose adjustment in patients with kidney disease involves increasing the dosing interval or reducing the dose.
GFR is the key clinical measure of kidney function. In general, for drugs that are excreted by the kidney, a decrease in GFR is associated with a decrease in drug clearance and the dosage needs to be reduced.
The GFR can be quantitated in multiple ways and each has advantages and disadvantages. The measured GFR (mGFR) is the gold standard but it is resource intensive and expensive, so the estimated GFR (eGFR) is used to classify and monitor the severity of chronic kidney disease (Table 1).
Table 1 - Relationship between glomerular filtration rate and stage of chronic kidney disease*
|
Kidney function stage |
eGFR (mL/min/1.73 m2) |
|
1 | ≥90 |
|
2 |
60–89 |
|
3a |
45–59 |
|
3b |
30–44 |
|
4 |
15–29 |
|
5 |
<15 or on dialysis |
eGFR estimated glomerular filtration rate
* The stage of chronic kidney disease is not only based on eGFR, but also on an assessment of kidney damage (eg. proteinuria, haematuria)
GFR can be assessed using serum creatinine-based formulae – Cockcroft-Gault6 and CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration)7. Since creatinine is an end product of muscle breakdown, each formula allows for the serum creatinine concentration to be adjusted for body mass based on patient characteristics.
The Cockcroft-Gault formula estimates creatinine clearance (eCrCl) and incorporates age, sex and body weight (Box 1).6 Because eCrCl was validated against measured CrCl based on 24-hour urine collection, it overestimates the actual GFR given that creatinine is both filtered and secreted in the nephron tubules. The usual units for eCrCl are mL/minute and multiple online calculators are available. However, by 2010 most laboratories in Australia were using a newer creatinine assay standardised to isotope dilution mass spectrometry (IDMS) which resulted in a 10–20% decrease in creatinine concentrations. This, in turn, will increase the eCrCl compared to what would have been calculated pre-2010.
The CKD-EPI formula estimates GFR because it was validated against GFR measured using exogenous filtration markers.7 It incorporates age and sex into a relatively complicated formula. These demographics are known at the time of blood collection so the eGFR is automatically calculated and reported by the laboratory. The units for the automated eGFR are mL/min/1.73 m2 and it is now an accepted method for the classification and monitoring of chronic kidney disease (Table 1).8,9
The initial report describing the CKD-EPI formula did not observe an effect of age or body mass index (BMI) on the accuracy of its prediction.7 However, it should be noted that the initial report was based on a population who were mostly younger than 66 years old with a mean body surface area of 1.90–1.93 m2 and a BMI of 27–28 kg/m2 (mean height 170 cm, mean weight 79–82 kg). The automated eGFR may not therefore apply to patients with different demographics. Since the body surface area for most patients is higher than 1.73 m2, the actual GFR in such a patient will be higher than that reported by the laboratory. The eGFR can be de-indexed (converted to actual mL/min) by multiplying the automated eGFR by the patient’s body surface area (m2) and then dividing by 1.73 (see Box 1).
The mGFR is determined after giving an exogenous filtration marker, such as 51Cr-EDTA, 125I-iothalamate, DTPA or MAG3. It is the most reliable method of quantifying GFR because these markers are filtered and not substantially secreted into or reabsorbed from the nephron. The mGFR can be indexed by adjusting for a standard body surface area of 1.73 m2.
The mGFR methods require parenteral administration of the exogenous marker and multiple blood and sometimes urine samples over time. The incremental gain from the mGFR above eGFR is uncertain in most cases, but they are used in specialist practice before a unilateral nephrectomy when considering the split GFR in each kidney.
Cystatin C is another endogenous solute that can be used to estimate GFR. However, the test is not universally offered by pathology laboratories in Australia at present.
Cystatin C is less influenced by muscle mass, so it may be advantageous in patients at extremes of body weight or those with cirrhosis. An alternative CKD-EPI formula has been developed to incorporate cystatin C.
There is debate about which formula – Cockcroft- Gault or CKD-EPI – is preferred for drug dosing because neither is a perfect representation of the true value of the GFR. There is debate about which formula – Cockcroft-Gault or CKD-EPI – is preferred for drug dosing because neither is a perfect representation of the true value of the GFR.
First, the criteria generally applied in developing these formulae are that the estimated value should be within 30% of the gold standard value (e.g. mGFR). For an eGFR or eCrCl in any patient at any time, the true GFR or CrCl could be nearly half or double that of the estimated value (so the absolute variability increases at higher GFRs, see Fig.). This significant uncertainty probably reduces the impact of the IDMS‑standardisation of creatinine assays on the calculated eCrCl.
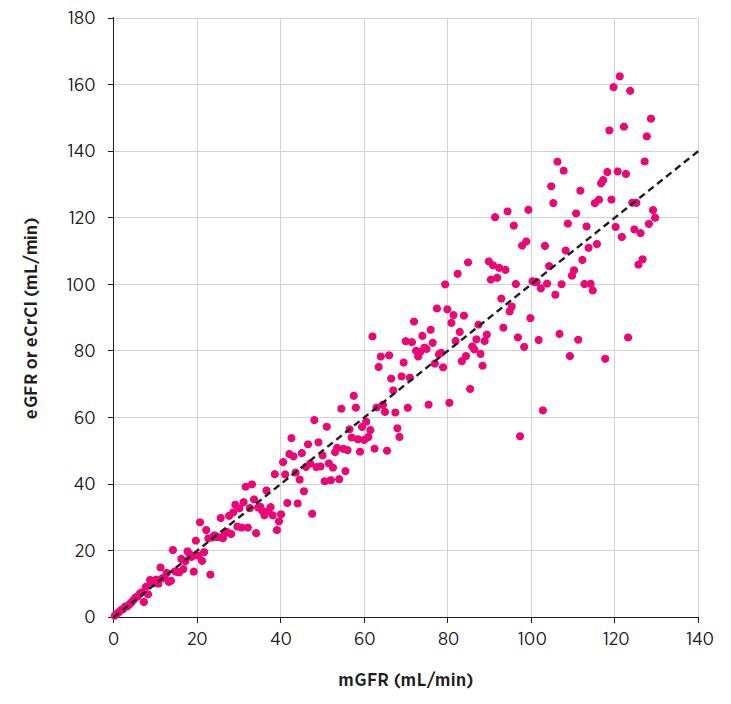
* The correlation of eGFR is imprecise, for example eGFR 30 mL/min may reflect an mGFR of 20–40 mL/min. The error on the prediction of mGFR from eGFR, and vice versa, increases at higher GFRs. Data based on simulation.
eCrCl estimated creatinine clearance
eGFR estimated glomerular filtration rate
mGFR measured glomerular filtration rate
Second, the eCrCl and automated eGFR do not give exactly the same results and eCrCl generally overestimates mGFR.10 For patients with a body surface area that is substantially different from 1.73 m2, the eGFR can be de-indexed to give units of mL/minute (Box 1). This value is used to inform drug dosing. For example, for the average patient enrolled in the study that developed the CKD-EPI formula,7 the mean actual GFR (mL/min) is approximately 10% higher than the automated eGFR, and more than 30% higher for those who are taller or heavier.
Some dosing recommendations are based on eCrCl so it is useful to understand how eGFR relates to eCrCl and the gold standard measurement mGFR.
The eGFR and eCrCl formulae were validated in people older than 18–20 years, and advancing age is associated with imprecision. For example, a study in patients over 60 years of age found that eCrCl and de-indexed eGFR were within 10% of each other in only 45% of cases and in most of these cases the eCrCl was lower than eGFR.11 The eCrCl was more likely to be lower in patients with a lower body weight (e.g. less than 60 kg) and increased age (e.g. older than 80 years).11 Unfortunately, mGFR was not measured in this study to assess the accuracy of the two serum creatinine-based formulae.
A study in 269 people aged 70 years and older noted that the absolute bias by eCrCl was less than that of de-indexed CKD-EPI (bias -3.2 ± 14.2 mL/min vs +7.1 ± 15.1 mL/min) compared to measured CrCl.12 However, another larger study (n=805) with a similar population except for a slightly higher average BMI found that the mean bias of de-indexed CKD-EPI was +2.7 mL/minute compared to mGFR,13 supporting the use of CKD-EPI.
In obese patients (BMI above 30 kg/m2), automated eGFR can underestimate GFR, and eCrCl based on actual body weight will overestimate GFR.10,14,15 In these patients, eCrCl based on adjusted ideal body weight (Box 1) or de-indexed eGFR are more reliable estimates of GFR14,15 (see Box 2 for an example). The opposite is true with eGFR for those who are underweight (BMI less than 18.5 kg/m2) with correction for body surface area resulting in a lower GFR estimate.10
The accuracy of these formulae may also vary depending on the GFR. For example, automated eGFR may be more accurate than indexed eCrCl at lower GFRs (e.g. less than 30 mL/min) and younger ages (e.g. under 40 years old).10
The impact of these patient characteristics on estimates of GFR are summarised in Table 2.
There are many other reasons why drug clearance (renal and non-renal) does not adequately correlate with creatinine-based measures of kidney function.5
Table 2 - Impact of patient characteristics on estimates of GFR
|
Patient characteristic |
eCrCl |
eGFR |
|
Reduced GFR |
May be less accurate |
May be more accurate |
|
Actual BSA >1.73 m2 |
Depends on body weight only, height is not incorporated |
Actual GFR is >30% higher for taller or heavier individuals |
|
Older age (>70 years) |
Acceptable |
Acceptable |
|
Younger age (<40 years) |
May be less accurate |
May be more accurate |
|
Obesity (e.g. BMI >30 kg/m2) or weight >120 kg |
Overestimates GFR, use adjusted ideal body weight |
Underestimates GFR, use de-indexed eGFR |
|
BMI <18.5 kg/m2 or weight <60 kg |
Acceptable, use actual body weight |
Overestimates GFR, use de-indexed eGFR |
eCrCl is estimated creatinine clearance as determined by the Cockcroft-Gault formula. The formula was validated against a 24-hour creatinine clearance and the units are mL/min. Actual body weight is commonly used in the calculations. The eCrCl is usually higher than the actual GFR.
eGFR is the estimated glomerular filtration rate as determined by the CKD-EPI formula. The formula was validated against a measured glomerular filtration rate and the units are mL/min/1.73 m2 body surface area.
BSA body surface area
BMI body mass index
GFR glomerular filtration rate
Despite these complexities and limitations, international and local expert groups support the use of automated eGFR to guide drug dosing.16 Overall, this appears reasonable given that potential benefits from a particular method (even if it was used to establish the therapeutic dose) are likely to be reduced in most cases due to inherent errors associated with any of these methods.
Drug information resources do not apply a consistent approach to the dosing of drugs in the context of kidney disease. For example, metformin and rivaroxaban dosing is based on creatinine clearance (presumably Cockcroft-Gault eCrCl), eplerenone on eGFR, and tranexamic acid on eGFR or serum creatinine depending on the resource. For lithium or sotalol, guidance for dose reduction is generally vague and a conservative approach is recommended for initial dosing and up-titration.
Small deviations in eGFR are not likely to be clinically meaningful and should not lead to an immediate dose adjustment (or cessation) but instead prompt ongoing monitoring of kidney function.
A more careful approach may be warranted for drugs with a narrow therapeutic index. This is particularly the case if the patient’s eGFR is close to a threshold prompting dose adjustment, the patient has a body surface area that differs significantly from 1.73 m2, and the drug requires a minimum concentration to be effective (e.g. antimicrobials). In such cases, the eGFR should be corrected (de-indexed) for the body surface area, and drug efficacy and toxicity should be monitored. Therapeutic drug monitoring is also useful for some medicines such as digoxin, lithium and potentially oral anticoagulants.
Automated eGFR is an adequate measure of kidney function for drug dosing in most cases, but there are notable exceptions requiring further consideration. Dose adjustment in chronic kidney disease always requires decision making on a case-by-case basis. Alternative laboratory methods for guiding drug dosing are being researched, such as tests based on cystatin C, and may have a useful role in the future.
Darren Roberts is the Chair of the Editorial Executive Committee of Australian Prescriber.
Acknowledgement: Darren Roberts acknowledges support of the Clinician ‘Buy-Out’ Program, St Vincent’s Centre for Applied Medical Research.
Australian Prescriber welcomes Feedback


