Article
Hyperprolactinaemia
- Angela X Chen, Morton G Burt
- Aust Prescr 2017;40:220-4
- 1 December 2017
- DOI: 10.18773/austprescr.2017.060
Serum prolactin should only be measured in patients with a pituitary mass or the clinical symptoms and signs of hyperprolactinaemia.
There are many causes of hyperprolactinaemia, including drugs. It is important to identify the underlying cause to guide appropriate treatment.
Hyperprolactinaemia can cause galactorrhoea and impair reproductive function. It can accelerate bone loss if it is associated with sex hormone deficiency.
Most prolactinomas are microprolactinomas. They usually do not grow sufficiently to cause hypopituitarism or visual field loss.
Patients with a prolactinoma are usually successfully treated with a dopamine agonist such as cabergoline.
A high prolactin concentration in blood (hyperprolactinaemia) is a relatively common endocrine abnormality. The causes range from benign conditions requiring no treatment to major medical problems necessitating immediate therapy. Hyperprolactinaemia can also be an adverse effect of some drugs.
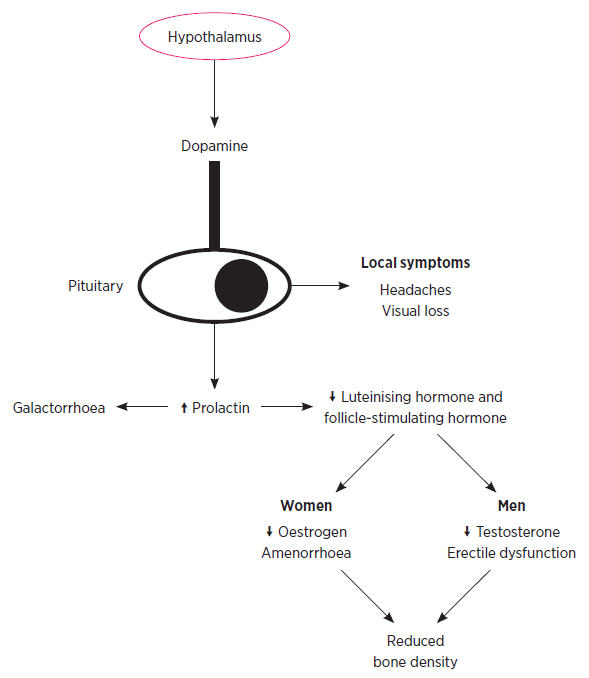
Prolactin is a polypeptide hormone that is synthesised and secreted by lactotroph cells in the anterior pituitary gland. The secretion of prolactin is primarily regulated by dopamine, which is produced in the hypothalamus and inhibits prolactin secretion. The hypothalamic hormone thyrotropin-releasing hormone stimulates prolactin secretion.
Prolactin exerts its effects by binding to prolactin receptors. These are located on the cell membrane of many cells, particularly in the breast and pituitary. In the breast, prolactin stimulates glandular proliferation during pregnancy and breast milk production postpartum. In the pituitary gland, prolactin inhibits gonadotrophin secretion.
There are physiological, pathological and drug-related causes of hyperprolactinaemia (Table 1).
Table 1 - Causes of hyperprolactinaemia
Examples |
|
|---|---|
Physiological (transient hyperprolactinaemia) |
Pregnancy |
Macroprolactinaemia |
Immunoglobulin (IgG) binding prolactin |
Hypothalamic/ pituitary lesions |
Prolactinoma
Inflammatory/infiltrative lesions:
|
Other illness |
Hypothyroidism |
Drugs |
Antipsychotics (risperidone, amisulpride, paliperidone, haloperidol) |
Pregnancy, suckling and lactation, exercise, coitus and stress can all increase prolactin. These increases are transient, and usually do not exceed twice the upper limit of normal reference ranges.
Estimates suggest that at least 10% of hyperprolactinaemia is secondary to macroprolactinaemia.1 This arises when immunoglobulins in serum bind prolactin to create high-molecular-weight forms of prolactin. As clearance of these macroprolactin molecules is slower than monomeric prolactin, the serum prolactin concentration increases. Macroprolactin is largely biologically inactive, so most patients with macroprolactinaemia are asymptomatic.
Prolactinomas are tumours arising from the prolactin secreting cells in the pituitary. Most prolactinomas (90%) are microadenomas (<1 cm in diameter), which are 10 times more common in women than in men. Microadenomas cause a moderate elevation in prolactin that can be associated with symptoms of hyperprolactinaemia, but they usually do not grow and cause a mass effect or hypopituitarism.2
Macroadenomas (>1 cm in diameter) are less common and giant prolactinomas (>4 cm in diameter) are rare. Compared with women, men are nine times more likely to present with a macroadenoma. These tumours cause marked hyperprolactinaemia – a prolactin concentration more than 10 000 mIU/L almost always indicates a macroprolactinoma. They can cause hypopituitarism and visual field loss or ocular palsies by compressing the optic chiasm or the cranial nerve nuclei.
Other hypothalamic and pituitary masses can also cause hyperprolactinaemia. As dopamine inhibits prolactin secretion, any mass or infiltrative lesion that compresses the pituitary stalk can attenuate dopamine’s action and cause hyperprolactinaemia. However, hyperprolactinaemia from stalk compression is usually below 2000 mIU/L, allowing distinction from a macroprolactinoma.3
Several illnesses can cause hyperprolactinaemia. Prolactin is predominantly renally cleared, so renal impairment can increase prolactin concentration. As thyrotropin-releasing hormone stimulates prolactin secretion, hypothyroidism can also cause hyperprolactinaemia. Seizures can cause a transient increase in prolactin.
A number of drugs impair hypothalamic dopamine release leading to increased secretion of prolactin (prolactin 500–4000 mIU/L). Hyperprolactinaemia develops in patients taking antipsychotics such as risperidone. It can also develop, to a lesser extent, with some selective serotonin reuptake inhibitors.4,5 Other drugs may cause hyperprolactinaemia less frequently (Table 1). If hyperprolactinaemia is drug-induced, concentrations usually normalise if the drug is ceased for 72 hours.
In some patients hyperprolactinaemia causes no symptoms, but it can affect breast and reproductive function (Table 2 and Fig. 1). In women, it can cause oligo-amenorrhoea, infertility and galactorrhoea. In men, hyperprolactinaemia can result in erectile dysfunction, infertility and gynaecomastia. Galactorrhoea is much less common in men than in women.6 In both sexes, gonadal hormone deficiency can accelerate bone loss. Patients may present with symptoms or signs associated with the underlying cause of hyperprolactinaemia. For example, headache and visual loss in a patient with a pituitary mass, and fatigue and cold intolerance in a patient with hypothyroidism.
Table 2 - Clinical features of hyperprolactinaemia
| Women | Men | |
|---|---|---|
Breast |
Galactorrhoea |
Gynaecomastia |
Reproductive |
Oligo-amenorrhoea |
Erectile dysfunction |
It should be emphasised that prolactin should only be measured in patients with clinical symptoms or signs of hyperprolactinaemia or patients with a known pituitary mass.
The diagnosis of hyperprolactinaemia can be based on a single measurement of serum prolactin that is above the upper limit of normal. The venepuncture must be performed without excessive stress.5
Macroprolactinaemia should be excluded, especially in asymptomatic patients, by adding polyethylene glycol to a serum sample to precipitate macroprolactin.5 Many laboratories in Australia routinely screen for macroprolactin in cases of apparent hyperprolactinaemia. Polyethylene glycol precipitation also allows for the measurement of monomeric prolactin, which is usually normal in patients with macroprolactinaemia.
Once the diagnosis of hyperprolactinaemia has been made, investigations are required to identify the underlying cause and associated complications. Women and men should have oestrogen and morning testosterone measured respectively along with gonadotrophins. Thyroid and renal function should be assessed and pregnancy excluded in women of childbearing age.
Unless another clear cause is identified, MRI of the pituitary is indicated. Patients with a pituitary mass more than 1 cm in diameter should have investigations assessing other pituitary hormones and have visual field testing. Measure the bone mineral density of hypogonadal patients.
Some patients do not require treatment. Patients with physiological hyperprolactinaemia, macroprolactinaemia, asymptomatic microprolactinoma or drug-induced hyperprolactinaemia usually do not require treatment. If hyperprolactinaemia is secondary to hypothyroidism, treating the patient with thyroxine should normalise prolactin.
In patients with symptomatic drug-induced hyperprolactinaemia the first consideration is whether the drug can be withdrawn, or replaced with an alternative that does not cause hyperprolactinaemia. If the risks of stopping the drug are greater than the potential benefits, any hypogonadism can be treated with appropriate sex hormone replacement. Occasionally patients with galactorrhoea can be prescribed a dopamine agonist, but this may impair the primary action of the drug which has caused the hyperprolactinaemia. For example, prescribing a dopamine agonist to a patient taking an antipsychotic drug could exacerbate their psychiatric condition.
The first-line treatment of a prolactinoma is a dopamine agonist. These are recommended in all patients with a macroprolactinoma and most patients with a symptomatic microprolactinoma. The two most commonly used dopamine agonists in Australia are cabergoline and bromocriptine. Both drugs should be started at a low dose and titrated up as required to minimise gastrointestinal adverse effects and orthostatic hypotension. A third option, quinagolide, is a non-ergot-based dopamine agonist that is also available in Australia.
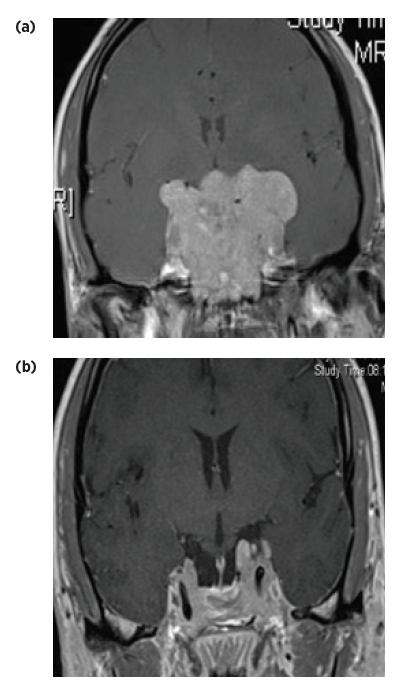
Bromocriptine is a non-selective dopamine agonist that binds to D1 receptors in the gut and D2 receptors in the pituitary. Cabergoline has a longer half-life and is more specific for the D2 receptors. Consequently, cabergoline is more effective and better tolerated than bromocriptine and is the recommended first-line treatment.5,7 Cabergoline normalises prolactin in up to 95% of patients, reduces tumour size in about 90% and controls symptoms in the majority of patients.5 It can be extremely effective, even in a patient with a giant prolactinoma (Fig. 2). Correction of sex hormone deficiency also improves bone mineral density, although bisphosphonate therapy can occasionally be required.
Treatment resistance is defined as a less than 50% reduction in tumour size or a prolactin concentration that does not return to normal with dopamine agonist therapy. It occurs in 10% of patients with a prolactinoma treated with cabergoline and in 25% of those treated with bromocriptine.5 In these patients, an alternative dopamine agonist or higher than usual doses can be trialled. Patients with persistent visual field defects, dopamine agonist resistance and pituitary apoplexy* often require transsphenoidal surgery, radiotherapy or both. Following surgery, prolactin normalises in approximately 90% of patients with microadenomas but in less than 50% of patients with macroadenomas.5
In addition to D2 receptors, cabergoline has high affinity for serotonin 2B (5-HT2B) receptors on cardiac valves. Consequently, cabergoline has been associated with cardiac valvulopathy in patients with Parkinson’s disease,8 but this adverse effect is mainly when daily doses are above 3 mg.8 Most patients with prolactinoma require much lower doses, for example less than 2 mg/week. The available evidence suggests that these lower doses of cabergoline do not cause valvulopathy.5 Bromocriptine does not activate the 5-HT2B receptor so does not cause valvulopathy.
Prolactin should be measured one month after starting a dopamine agonist and periodically thereafter. Pituitary MRI is often repeated after one year of therapy in patients with a microprolactinoma.5 It should be repeated earlier in patients with a macroprolactinoma, new symptoms or a progressive increase in prolactin concentration despite treatment. Visual fields and bone density should be reassessed if they were abnormal before treatment.
Dopamine agonists can often be stopped after 2–3 years of dopamine agonist treatment in patients who maintain a normal prolactin concentration during gradual tapering of the dopamine agonist dose, especially if there is no visible adenoma on MRI.5 However, the risk of recurrent hyperprolactinaemia ranges from 26–69%. Recurrence is usually during the first 12 months after treatment cessation, therefore serum prolactin must be regularly monitored after treatment withdrawal.6,9
In women, dopamine agonist therapy usually restores ovulation and fertility. The oestrogen concentration increases during pregnancy and causes clinically significant growth in 20–25% of macroprolactinomas. However, the risk of significant enlargement of a microprolactinoma is only about 3%.
There is no evidence that bromocriptine or cabergoline are associated with adverse outcomes in pregnancy, however in women with a microadenoma, dopamine agonists are usually stopped when pregnancy is confirmed. As the prolactin concentration rises during normal pregnancy, serial prolactin measurement is not informative. Patients should be monitored for clinical signs, such as visual field loss, which suggest the tumour is growing. MRI and visual field testing can be performed if there are concerns.
In patients with a macroadenoma the decision whether to stop a dopamine agonist during pregnancy should be individualised. They should undergo regular clinical review and visual fields should be formally assessed every three months.
Hyperprolactinaemia is a common occurrence encountered in clinical practice. Investigations are needed to find the cause of hyperprolactinaemia to guide appropriate treatment. Symptomatic patients with a prolactinoma are usually treated with the dopamine agonist cabergoline. This effectively normalises prolactin and reduces the size of the prolactinoma in the majority of patients.
Morton Burt was previously awarded a competitive Pfizer cardiovascular lipid research grant.
* Pituitary apoplexy is an emergency caused by acute haemorrhage or infarction in the pituitary gland. Symptoms may include severe headache and altered vision.

