Article
Limiting antipsychotic drugs in dementia
- Stephen Macfarlane, Colm Cunningham
- Aust Prescr 2021;44:8-11
- 1 February 2021
- DOI: 10.18773/austprescr.2020.078
Most patients with dementia have behavioural and psychological symptoms. The first-line treatments for these symptoms are not drugs, but behavioural and psychological interventions.
Antipsychotic drugs are widely prescribed for people living with dementia. This is despite a high adverse effect burden and limited evidence of efficacy.
Most behavioural and psychological symptoms will subside spontaneously within six months. Trials of deprescribing are therefore recommended.
Behaviours should be seen as symptoms that have an underlying cause. Treatment should target these causes, rather than the resultant behaviours.
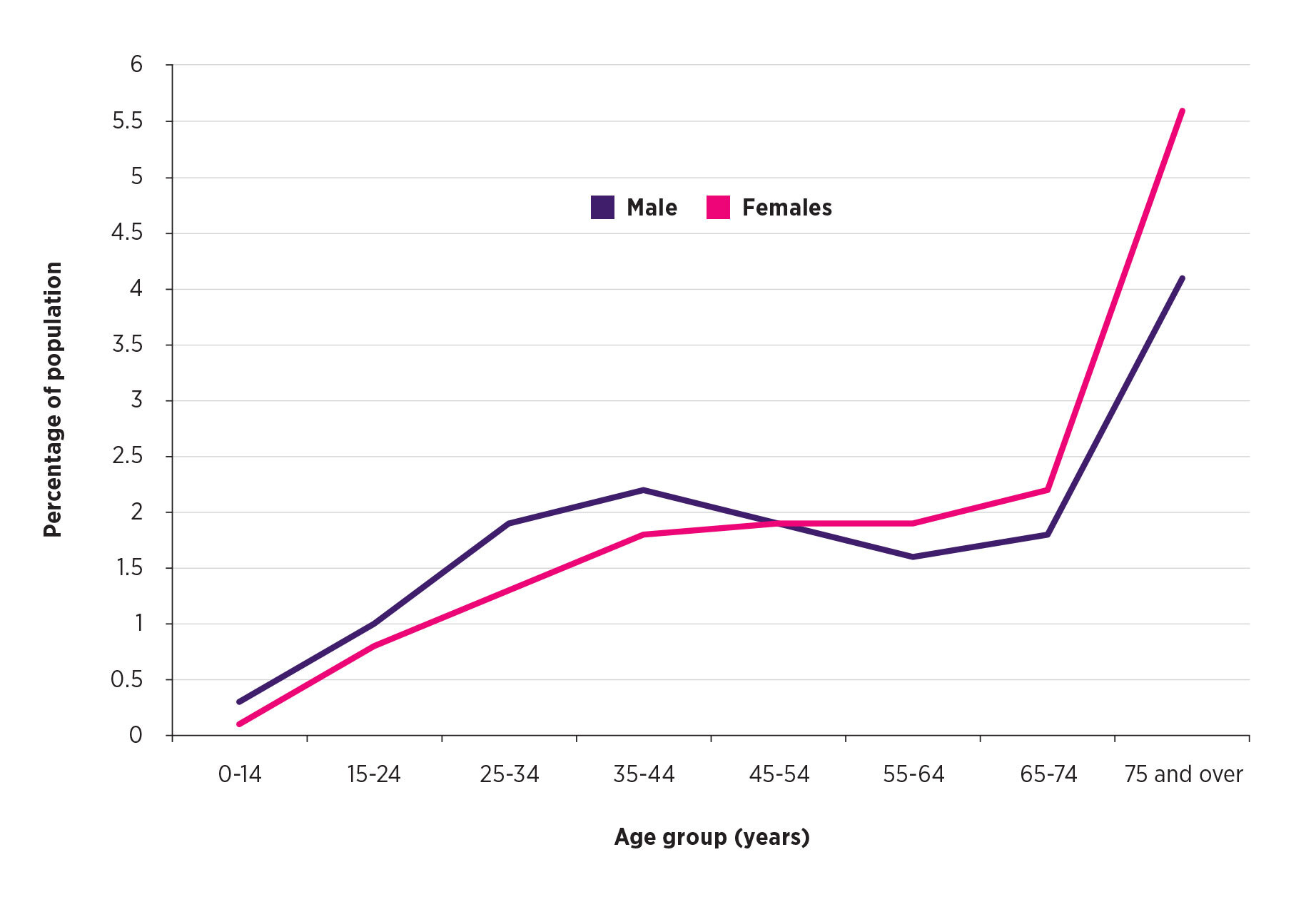
Older people are prescribed psychotropic drugs at a rate that dwarfs that of younger cohorts (Fig. 1).1,2 Much of this prescribing occurs in residential care settings. The prevalence of antipsychotic use may be up to 44% in this population.3 A large proportion of antipsychotic prescribing occurs in the three months before someone enters aged care. It then increases markedly in the three months after admission.4 These drugs are often prescribed for the management of the behavioural and psychological symptoms of dementia. This is despite a lack of efficacy and high rates of adverse effects.5 It has been estimated that only 10% of psychotropic prescribing for those living with dementia is appropriate.6
Many behaviours that can occur in dementia are unlikely to respond to pharmacotherapy at all. For example, there is no drug treatment for wandering, or calling out. A drug cannot be expected to modify behaviours such as shadowing staff, exit-seeking, disrobing or inappropriate voiding. In such cases, the only means by which an antipsychotic may have efficacy is by sedating the person to the point where they are no longer able to engage in such behaviours. This constitutes chemical restraint.
Placebo response rates in randomised controlled trials of antipsychotics for behavioural and psychological symptoms of dementia are high. This reflects the high rate of spontaneous remission of all these types of symptoms within three months.7 When an antipsychotic has been prescribed and a behaviour subsequently resolves, it may be tempting to conclude that this is because of the drug, however the behaviour may well have settled without the drug.
The behaviours for which antipsychotics may have some benefit are limited to psychosis, agitation and aggression. However, apart from psychosis, the mechanism of action is unclear, so the effects may also represent non-specific sedation.
In Australia, risperidone is the only antipsychotic approved for the treatment of behavioural and psychological symptoms of dementia. However, there are data that other antipsychotics are frequently prescribed off label for the behavioural and psychological symptoms of dementia.8 The Pharmaceutical Benefits Scheme restricts the use of risperidone to behavioural symptoms characterised by psychosis and aggression in those with Alzheimer’s disease, for a 12-week period, and only after non-pharmacological interventions have failed. While there is evidence that risperidone can benefit the specific behavioural and psychological symptoms of agitation and aggression, the effect sizes are small.9
The adverse effect burden of antipsychotic drugs is significant and includes falls, sedation, extrapyramidal adverse effects and death. These problems are often treatment-emergent and related not only to dose, but duration of exposure, underlining the need for frequent monitoring for adverse effects. The limited efficacy of antipsychotics, combined with their poor tolerability and safety profile, makes the obtaining of consent vital before starting any treatment. An assessment of an individual’s capacity to refuse treatment must always be made before seeking proxy consent from an authorised decision maker.
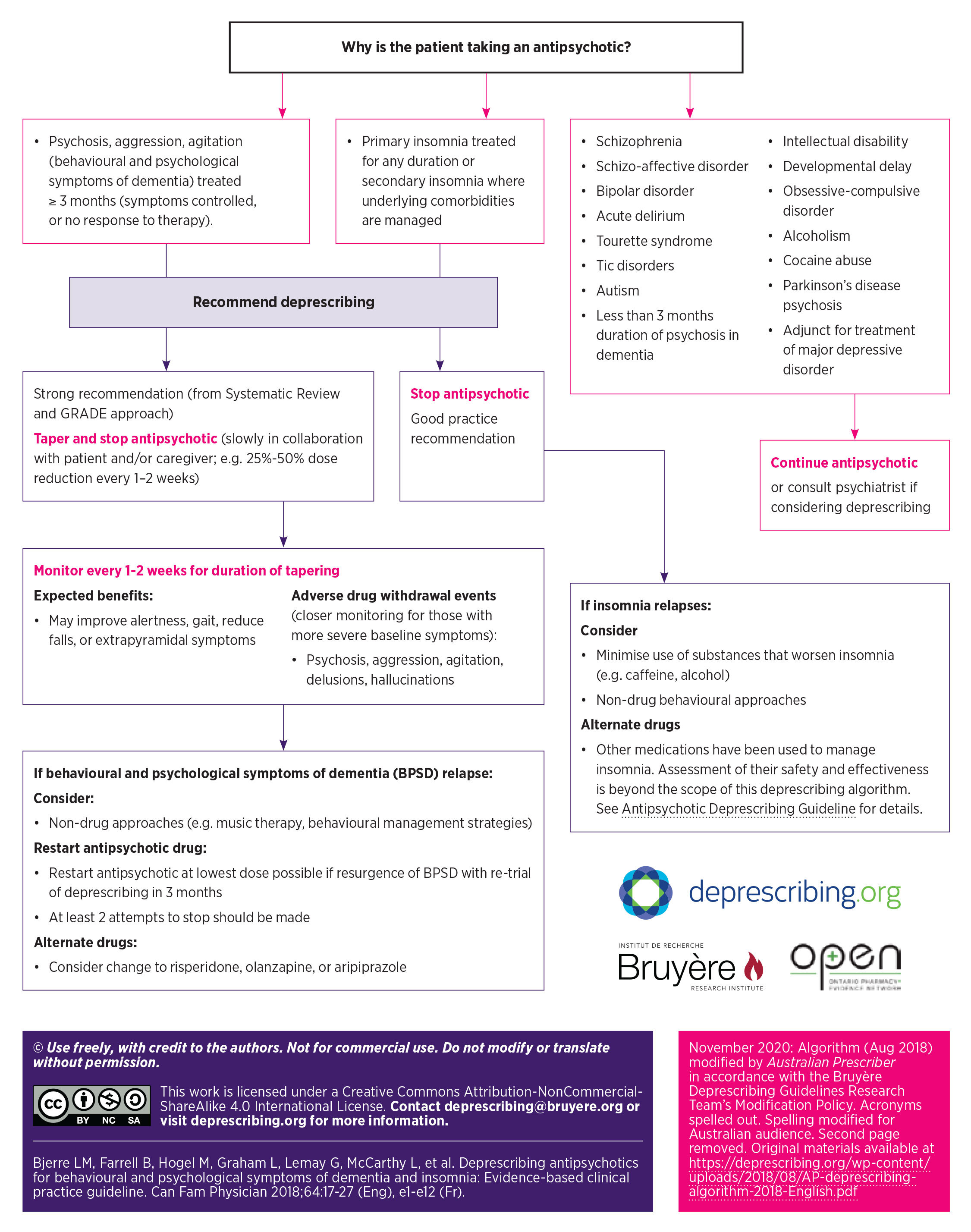
A deprescribing plan should be provided when starting an antipsychotic drug in a patient with dementia. If an antipsychotic has been prescribed and the symptoms settle, a trial of deprescribing is warranted. Figure 2 shows an algorithm as to how deprescribing might be approached.10 It is important to involve other members of the multidisciplinary team such as nurses and a pharmacist in the development of a deprescribing plan. Deprescribing provides an ideal opportunity to try specific non-drug strategies for any behaviours that might re-emerge as the drug is withdrawn.
It is important to identify what may be causing the behavioural and psychological symptoms in someone with dementia. Agitation and aggression are symptoms, not diagnoses. Just because a drug may have efficacy in treating agitation does not mean that the drug is indicated in response to the symptom. The key to developing effective non-pharmacological interventions is an accurate assessment of the cause of the behavioural symptoms. Appropriate management cannot occur in the absence of adequate assessment.
Common causes of symptoms include unrecognised or undertreated pain, depression, and delirium. Expert consensus for the pharmacotherapy of behavioural and psychological symptoms of dementia emphasises trials of analgesia and antidepressants before considering antipsychotic use.11 If an antipsychotic is going to be used, the need for continuing analgesics and antidepressants should be reviewed.
The Commonwealth Government has funded free, national dementia behaviour-management services since 2007. The various state and territory-based services were united under a single provider, Dementia Support Australia, in 2016. This has a multidisciplinary workforce with expertise in the assessment and non-pharmacological management of the behavioural and psychological symptoms of dementia. It is backed by a national team of geriatricians and old-age psychiatrists. Referrals can be made via 1800 699 799 or online.
The evidence for the efficacy of antipsychotic drugs in the treatment of behavioural and psychological symptoms of dementia is unconvincing. However, the drugs cause definite harm including an increased risk of death.
The common medical causes of altered behaviour in someone with dementia should be identified. More detailed evaluation and the subsequent development of individualised behaviour-management plans can involve referral to a multidisciplinary team with experience in the area.
Conflicts of interest: Stephen Macfarlane has received research funding from Janssen-Cilag, Eli Lilly, Eisai, Roche, Anavex Life Sciences, Prana Biotechnology, Alector, Sanofi, Pfizer, Forest, Velacor, Lundbeck, Cognition Therapeutics, Genentech. Speakers’ honoraria have been provided by Eli Lilly, Janssen, Pfizer and Lundbeck. Stephen Macfarlane has served on a Scientific Advisory Board for Eli Lilly. He is an employee of Dementia Support Australia.
Australian Prescriber welcomes Feedback.
Head of Clinical Governance, Dementia Centre, HammondCare, Sydney
Head of Clinical Governance, Faculty of Medicine and Health Sciences, Monash University, Clayton, Victoria
Director, Dementia Centre, HammondCare, Sydney
Associate professor, School of Public Health and Community Medicine, University of New South Wales, Sydney

