Article
Thyroid disorders in pregnancy and postpartum
- Ashleigh Smith, Jade Eccles-Smith, Michael d’Emden, Karin Lust
- Aust Prescr 2017;40:214-9
- 1 December 2017
- DOI: 10.18773/austprescr.2017.075
Thyroid dysfunction in pregnancy has consequences for mother and baby. Potential problems include pre-eclampsia, prematurity and congenital abnormality.
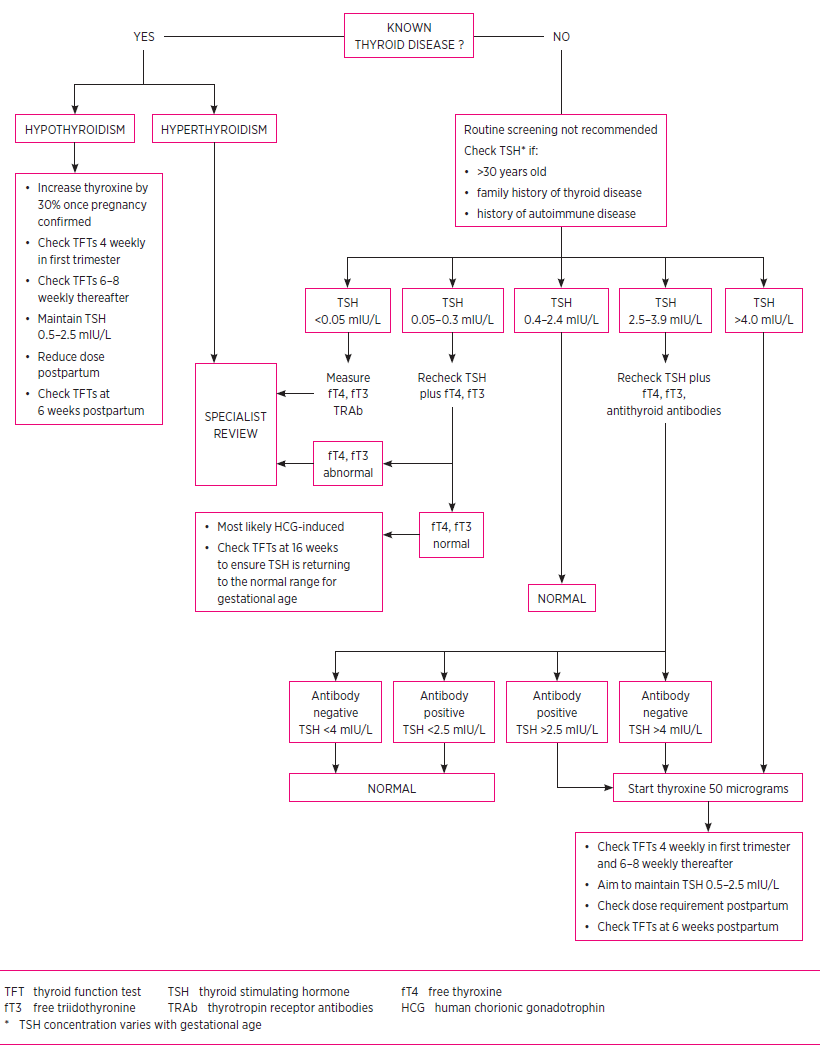
For women known to have hypothyroidism, an increase in thyroxine dose by 20–40% when pregnancy is confirmed usually ensures they remain euthyroid. Treatment of subclinical hypothyroidism is recommended if the woman has antithyroid antibodies.
Treatment of hyperthyroidism, unless it is related to human chorionic gonadotrophin, involves propylthiouracil in the first trimester. Carbimazole may be used in the second trimester. Thyroid function tests are checked every month and every two weeks following a change in dose.
Women with a current or a past history of Graves’ disease who have thyrotropin receptor antibodies require early specialist referral as there is a 1–5% risk of fetal hyperthyroidism.
Women with thyroid disorders in pregnancy should be followed up by their GP in the postpartum period. Postpartum thyroiditis may present months after delivery.
During pregnancy the thyroid gland undergoes hyperplasia and increased vascularity. Circulating iodine is reduced and thyroid-binding globulin increases.
The rising concentration of beta-human chorionic gonadotrophin (HCG) in the first trimester can directly stimulate the thyroid stimulating hormone (TSH) receptor as HCG has structural similarities to TSH. This in turn leads to increased free triidothyronine (fT3) and free thyroxine (fT4), suppressing TSH secretion. A serum TSH below 0.1 mIU/L may be present in 5% of women by the 11th week of pregnancy.
The TSH subsequently normalises as beta-HCG falls in the second and third trimesters.
In view of these physiological changes, consult gestation-specific TSH concentration ranges when interpreting thyroid function tests. These reference ranges differ from non-pregnant ranges (Table 2).7,8
The fetal thyroid starts functioning at 10–12 weeks gestation but does not fully mature until the third trimester. Before then the fetal metabolic requirements are met by maternal thyroxine.
Women have an increased iodine requirement during pregnancy and lactation due to increased thyroid hormone production, increased renal iodine excretion and fetal iodine requirements. The National Health and Medical Research Council recommends pregnant and breastfeeding women take a daily supplement of iodine 150 micrograms. The recommended total daily intake of iodine in pregnancy is 250 micrograms.9
For women with overt hypothyroidism who are planning pregnancy, guidelines recommend optimisation of TSH before conception. Thyroid dysfunction in pregnancy is clinically important as insufficient thyroxine is associated with an increased risk of premature birth, low birth weight and miscarriage.2,4,5
After conception, an increase in thyroxine as soon as possible is recommended with the goal of normalising the TSH concentration. An easy approach is to increase the total weekly thyroxine dose by an extra two tablets per week or by 20–30% of the baseline dose when pregnancy is confirmed.6,8,10
Serum TSH should be monitored every four weeks in the first trimester to ensure the woman is euthyroid, and then six to eight weekly therafter.11 Thyroid function tests should be rechecked four weeks after any dosage adjustments to ensure euthyroid levels are maintained. Aim to maintain TSH in the range 0.5–2.5 mIU/L.
Failure to achieve a euthyroid state despite appropriate therapy necessitates investigation into causes for a lack of thyroxine uptake. This can result from poor adherence to therapy or impaired absorption. Women should be advised to take their thyroxine on an empty stomach before breakfast. There should be a 4–5 hour gap before taking medicines such as vitamins, calcium and iron tablets as interactions in the gastrointestinal tract can reduce thyroxine absorption.
Following delivery, the thyroxine dose should be reduced to the patient’s preconception dose, assuming the woman was euthyroid on that dose. Check thyroid function tests 4–6 weeks after their dose has been reduced postpartum.8
A new diagnosis of overt hypothyroidism should warrant immediate thyroxine replacement and further investigation for the presence of thyroid auto antibodies:
The usual starting dose of thyroxine is at least 50 micrograms per day with maintenance between 100 and 150 micrograms per day.11,12 The starting dose of thyroxine will depend on the degree of hypothyroidism,13 the size of the patient and the presence of other medical problems. If unsure, the most important thing is to check thyroid function soon after starting therapy (e.g. at 4 weeks) and up-titrate the dose aiming to achieve a TSH below 2.5 mIU/L as quickly as possible.
Subclinical hypothyroidism in pregnancy is associated with an increased risk of recurrent miscarriage, intrauterine growth restriction, preterm birth, low birth weight, perinatal mortality and pre-eclampsia.14-17 Thyroxine may reduce associated risks.18 Recent studies support thyroxine replacement in women with subclinical hypothyroidism undergoing assisted reproduction technologies, to improve pregnancy outcome.6,19,20 The aim of treatment is to achieve a TSH less than 2.5 mIU/L.
Women with subclinical hypothyroidism should be tested for antithyroid antibodies as this impacts on the effects in pregnancy and may also be associated with other autoimmune conditions such as type 1 diabetes.6,7 At present there are no data to support treating pregnant women who have subclinical hypothyroidism if they do not have antibodies.
Previous guidelines recommended giving thyroxine to all women with subclinical hypothyroidism, regardless of their antibody status.11 This was due to research which reported multiple maternal and neonatal adverse outcomes associated with subclinical hypothyroidism, however the role of thyroxine therapy in preventing these outcomes was unclear.21
The American Thyroid Association in 2017 updated its guidelines for the management of thyroid disease in pregnancy following new research. Thyroxine should be given if there are antithyroid antibodies and the initial TSH is 2.5–4 mIU/L. If the initial TSH is 4 mIU/L or more, start thyroxine irrespective of antibody status.6
If a decision is made to treat subclinical hypothyroidism, the suggested starting dose of thyroxine is 50 micrograms per day. Thyroid function tests are checked within four weeks of starting therapy.11,12
In the postpartum period the ongoing need for thyroxine needs to be reassessed. The concentrations of thyroid hormones that prompted treatment during pregnancy may be satisfactory in a non-pregnant woman. If the woman had antithyroid antibodies but the initial TSH was less than 4 mIU/L, cease thyroxine and recheck thyroid function at six weeks. If the TSH was greater than 4 mIU/L continue thyroxine. In women who did not have antithyroid antibodies but had TSH greater than 4 mIU/L, cease thyroxine and check thyroid function in six weeks.6
Targeted screening is reported to miss up to 30% of cases of thyroid dysfunction. A recent study reported 9.6% of cases of subclinical hypothyroidism would have been missed by targeted screening. If prospective trials find that treating subclinical hypothyroidism in pregnancy is beneficial, this would support universal screening in future.22
Overt hyperthyroidism in pregnancy has a prevalence of 0.1–0.4%.1 Graves’ disease accounts for 85% of these cases, followed by HCG-mediated hyperthyroidism.1 Rarer causes include toxic multinodular goitre, thyroiditis and toxic adenoma.2,23 The presence of thyrotropin receptor antibodies distinguishes Graves’ disease from HCG-mediated hyperthyroidism. This is important as they have different risks of fetal hyperthyroidism and require different management.
Nuclear medicine thyroid radioiodine scans are contraindicated in pregnancy due to the risk to the fetus. They should not be used to investigate hyperthyroidism in pregnancy.
HCG-mediated hyperthyroidism (TRAb negative) is usually transient and related to the physiological changes of pregnancy. Treatment is not generally required.10 Similarly, at present there is no evidence to support the treatment of subclinical hyperthyroidism in pregnancy.2 Observation with measurements of TSH and fT4 every four to six weeks is recommended as best practice.2
The circulating maternal thyrotropin receptor antibodies in Graves’ disease have the potential to cross the placenta and cause fetal hyperthyroidism.2 Maternal antibodies should be checked when pregnancy is confirmed, at 18–22 weeks and again at 30–34 weeks to evaluate the need for neonatal and postnatal monitoring. If the antibodies are elevated, the fetus will require monitoring for thyroid dysfunction with serial ultrasounds for fetal growth and signs of fetal hyperthyroidism.2,6,23
Medical therapy is recommended in women with overt hyperthyroidism due to Graves’ disease, toxic adenoma or toxic multinodular goitre.6 For these women the aims of therapy are to use the lowest dose of antithyroid drugs to minimise maternal and fetal adverse effects.6 The dose should be adjusted to keep maternal serum fT4 at the upper limit of the normal range to minimise the risk of fetal hypothyroidism.23
Both propylthiouracil and carbimazole cross the placenta and have implications in fetal development. The risks include fetal goitre and transient hypothyroidism.2,24 Both drugs can cause maternal agranulocytosis.24
Propylthiouracil is recommended as the first-line antithyroid drug in the first trimester as carbimazole is associated with congenital abnormalities.
Start propylthiouracil at a dose appropriate for the severity of the hyperthyroidism after discussion with an endocrinologist or physician with experience in managing thyroid disease.2,6,23-24
If antithyroid medication is required after the first trimester, there is insufficient evidence at present to determine whether propylthiouracil should be changed to carbimazole. Both drugs are associated with rare but significant long-term adverse effects and it is unclear which has the greatest risk in the second trimester. Individual units may have specific management strategies. All women with Graves’ disease in pregnancy should be managed by a specialist in this area.2,6,23-24 If changing an antithyroid drug, assess thyroid function after two weeks, then return to four-weekly monitoring.2,23,24
Symptomatic treatment of tachycardia and tremors can be achieved with short-term use of a beta blocker (e.g. propranolol). As pregnancy progresses the dose of the antithyroid drug may be reduced and it can often be stopped.23
If the woman cannot be treated with antithyroid drugs, surgery may be indicated. It can be considered for women who are not adherent to the drugs, or who have had a severe adverse reaction and for those who require high doses (consider specialist referral at doses >30 mg/day carbimazole or >450 mg/day propylthiouracil). Ideally, surgery is performed in the second trimester.4
At delivery the paediatrician should be informed that the mother has been on antithyroid drugs, or has thyrotropin receptor antibodies as the neonate will require thyroid function monitoring.23 There is an increased risk of a recurrence of Graves’ disease in the postpartum period in women who ceased their antithyroid drug during pregnancy.23 Women can continue to use thyroxine or antithyroid drugs while breastfeeding.25
When a pregnant woman is found to have a thyroid nodule on examination it can be investigated with ultrasound. Imaging with radioactive iodine is contraindicated in pregnancy.
If the woman has a solid nodule smaller than 10 mm, it can usually be investigated after delivery. Ultrasound-guided fine-needle aspiration for cytology is indicated for larger lesions. Fine-needle aspiration should be considered for a nodule of 5 mm or more if the woman has a high risk of thyroid cancer or the ultrasound findings are suspicious for malignancy. Complex nodules 15 mm or larger also require fine-needle aspiration.
Some authors recommend that women near term (i.e. delivery in <4 weeks) could have fine-needle aspiration delayed until postpartum with probable safety.
If the biopsy is diagnostic or highly suspicious of malignancy, postponing surgery until postpartum is unlikely to change disease-specific survival in women with papillary or follicular neoplasm without evidence of advanced disease. However surgery could still be offered in the second trimester.2,23,26
Immediate surgery is indicated if the nodule causes tracheal obstruction.
Postpartum thyroiditis is defined as the development of hypothyroidism, thyrotoxicosis or both in the year following delivery, in any woman who did not have clinical evidence of thyroid disease before pregnancy.2 It occurs in 7–10% of postpartum women, although this varies depending on iodine intake and genetic factors.2
Investigation for postpartum thyroiditis is recommended if there is a clinical suspicion and it should be considered as a differential diagnosis in women presenting with depressive symptoms in the postpartum period. Almost 50% of women with antithyroid peroxidase antibodies in early pregnancy will develop postpartum thyroiditis, therefore it is the most useful marker identifying those at risk.27 Thyroid function tests are indicated at three and six months postpartum in these women and those with known autoimmune disease, previous postpartum thyroiditis or chronic viral hepatitis.2
Annual TSH tests for 5–10 years are recommended for women with a history of postpartum thyroiditis. They have an increased risk of developing permanent overt hypothyroidism.2
Thyroid dysfunction during pregnancy and the postpartum period is a common obstetric problem primarily managed by GPs. At-risk women are screened, but universal thyroid function screening is currently not recommended during pregnancy or postpartum.
Thyroxine is used for treating overt hypothyroidism and is recommended in antibody positive subclinical hypothyroidism. For hyperthyroidism, propylthiouracil is the preferred antithyroid drug in the preconception and first trimester to reduce the risk of teratogenicity.1 Carbimazole may be used in the second trimester.
Conflict of interest: none declared

Obstetrics and gynaecology registrar, Obstetrics and Gynaecology, Mater Mothers’ Hospital, South Brisbane
Basic physician trainee, Royal Brisbane and Women’s Hospital, Brisbane
Consultant endocrinologist, and Director Endocrinology and Diabetes, Royal Brisbane and Women’s Hospital, Brisbane
Consultant obstetric and General physician, and Interim clinical director Obstetrics and Gynaecology, Royal Brisbane and Women’s Hospital, Brisbane
