

What is in this leaflet
This leaflet answers some common questions about CANDESAN COMBI.
It does not contain all of the available information. It does not take the place of talking to your doctor or pharmacist.
All medicines have benefits and risks. Your doctor has weighed the risks of you taking CANDESAN COMBI against the benefits they expect it will have for you.
If you have any concerns about taking this medicine, talk to your doctor or pharmacist.
Keep this leaflet with your medicine. You may need to read it again.
What CANDESAN COMBI is used for
CANDESAN COMBI is used to treat high blood pressure, also called hypertension.
CANDESAN COMBI contains two medicines, candesartan cilexetil and hydrochlorothiazide. In combination, they lower your blood pressure more than using either one on its own.
Candesartan cilexetil belongs to a group of medicines known as angiotensin-II receptor antagonists. It works by relaxing the blood vessels.
Hydrochlorothiazide is type of medicine called a diuretic. It works by reducing the amount of excess fluid in the body.
Your doctor will have explained why you are being treated with Candesartan/hydrochlorothiazide tablets and told you what dose to take.
Your doctor may have prescribed CANDESAN COMBI for another reason.
Ask your doctor if you have any questions about why CANDESAN COMBI has been prescribed for you.
CANDESAN COMBI is available only with a doctor's prescription.
There is no evidence that CANDESAN COMBI is addictive
Before you take CANDESAN COMBI
When you must not take it
Do not take CANDESAN COMBI if you are allergic to:
- medicines containing candesartan cilexetil or hydrochlorothiazide
- other angiotensin II receptor antagonists (or blocker)
- any sulphur drugs (sulphonamides) such as some antibiotics or some medicines to treat diabetes
- any of the ingredients listed at the end of this leaflet.
Symptoms of an allergic reaction can include:
- shortness of breath,
- wheezing or difficulty breathing,
- swelling of the face, lips, tongue, or other parts of the body,
- rash, itching or hives on the skin.
Do not take CANDESAN COMBI if you have:
- severe kidney or liver disease and/or conditions associated with impaired bile flow (cholestasis)
- gout.
Do not use CANDESAN COMBI if you are taking blood pressure medicine containing aliskiren, especially if you have diabetes mellitus or have kidney problems.
Do not take CANDESAN COMBI if you are pregnant or are planning to become pregnant. CANDESAN COMBI may affect your developing baby if you take it during pregnancy.
Do not use CANDESAN COMBI if you are breastfeeding. Your baby can take in components of CANDESAN COMBI from breast milk if you are breastfeeding.
Do not give CANDESAN COMBI to children. There is no information about its use in children, so CANDESAN COMBI is not recommended for children.
Do not take CANDESAN COMBI if the expiry date (Exp.) printed on the pack has passed.
Do not take CANDESAN COMBI if the packaging is torn or shows signs of tampering. If it has expired or is damaged, return it to your pharmacist for disposal.
If you are not sure whether you should start taking this medicine, talk to your doctor.
Before you start to take it
Tell your doctor if you are allergic to any other medicines, foods, dyes or preservatives.
Tell your doctor if you have, or have had, any medical conditions, especially the following:
- kidney problems
- heart problems
- liver problems
- diabetes
- recent excessive vomiting or diarrhoea
- a salt reduced diet
- Systemic Lupus Erythematosus (SLE), a disease affecting the skin, joints and kidneys
- a condition called primary hyperaldosteronism
- a past operation known as sympathectomy.
- A decrease in vision or eye pain. These could be symptoms of fluid accumulation in the vascular layer of the eye (choroidal effusion) or an increase of pressure in your eye and can happen within hours to weeks of taking CANDESAN COMBI. This can lead to permanent vision loss, if not treated. If you earlier have had a penicillin or sulphonamide allergy, you can be at higher risk of developing this.
Experienced breathing or lung problems (including inflammation or fluid in the lungs) following hydrochlorothiazide intake in the past.
If you have not told your doctor about any of the above, tell them before you start taking CANDESAN COMBI.
Taking other medicines
Tell your doctor if you are taking any other medicines, including any that you buy without a prescription from a pharmacy, supermarket or health food shop.
Some medicines may be affected by CANDESAN COMBI, or may interfere with each other. These include:
- other blood pressure lowering medicines, particularly diuretics (fluid tablets) and ACE-inhibitors, especially if you have diabetes-related kidney problems
- medicines containing potassium, including salt substitutes
- digoxin, a medicine used to treat heart failure
- non-steroidal anti-inflammatory drugs (NSAIDS), medicines used to relieve pain, swelling and other symptoms of inflammation, including arthritis
- colestipol and cholestyramine, medicines used to treat high blood cholesterol levels
- lithium, a medicine used to treat mood swings and some types of depression
- alcohol
- strong pain killers, such as codeine, morphine, dextropropoxyphene
- barbiturates, used to treat epilepsy, such as phenobarbital (phanobarbitone)
- medicines like insulin that are used to treat diabetes
- Calcium supplements or medicines containing calcium
- Vitamin D supplements
- Medicines to treat irregular heart beats
- Corticosteroids such as prednisone, cortisone, dexamethasone
- Laxatives
- Medicines used to treat cancer such as cyclophosphamide
- Methotrexate, a medicine used to treat arthritis and some cancers
- Amantadine, a medicine used to treat Parkinson's disease
- Ciclosporin
These medicines may be affected by CANDESAN COMBI or may affect how it works. You may need different amounts of your medicines, or may need to take different medicines.
Your doctor and pharmacist have more information on medicines to be careful with or avoid while taking CANDESAN COMBI.
Things to be careful of
Move slowly when getting out of bed or standing up if you feel faint, dizzy or light-headed.
Be careful driving or operating machinery until you know how CANDESAN COMBI affects you.
You may feel dizzy when you start taking CANDESAN COMBI due to the drop in your blood pressure.
Drink plenty of water while you are using CANDESAN COMBI, especially if you sweat a lot.
Please talk to your doctor or pharmacist about these possibilities if you think they may bother you.
How to take CANDESAN COMBI
Follow all directions given to you by your doctor or pharmacist carefully. They may differ from the information contained in this leaflet.
If you do not understand the instructions on the box, ask your doctor or pharmacist for help.
How to take it
The usual dose is one tablet once daily, taken whole with a glass of water.
Take CANDESAN COMBI once a day, at about the same time each day.
Keeping a regular time for taking CANDESAN COMBI will help to remind you to take it.
It does not matter whether you take CANDESAN COMBI with food or on an empty stomach.
How long to take it
CANDESAN COMBI helps control your condition, but does not cure it.
Therefore you must take CANDESAN COMBI every day.
Continue taking the tablets for as long as your doctor tells you to.
If you forget to take CANDESAN COMBI
If you forget to take a dose, take it as soon as you remember, as long as it is at least 12 hours before your next dose is due. Then go back to taking it as you would normally.
If it is less than 12 hours to your next dose, skip the dose you missed and take your next dose when you are meant to.
Do not double the dose to make up for the dose you missed.
If you have trouble remembering when to take your medicine, ask your pharmacist for some hints.
If you take too much CANDESAN COMBI (overdose)
Immediately telephone your doctor, or the Poisons Information Centre (telephone 13 11 26), or go to Accident and Emergency at the nearest hospital, if you think you or anyone else may have taken too much CANDESAN COMBI. Do this even if there are no signs of discomfort or poisoning. You may need urgent medical attention.
If you take too much CANDESAN COMBI, you may get a headache and feel sick, dizzy, thirsty and very tired.
While you are taking CANDESAN COMBI
Things you must do
Take CANDESAN COMBI exactly as your doctor has told you to. Your blood pressure will not be well controlled if you do not.
If you are about to be started on any new medicine, remind your doctor and pharmacist that you are taking CANDESAN COMBI.
Tell all doctors, dentists and pharmacists who are treating you that you are taking CANDESAN COMBI.
Tell your doctor if you have excess vomiting and diarrhoea while taking CANDESAN COMBI. You may lose too much water and your blood pressure may become too low.
Tell your doctor immediately if you become pregnant or plan to become pregnant while taking CANDESAN COMBI. You should not use CANDESAN COMBI if you are pregnant or thinking about becoming pregnant. Your doctor can discuss different treatment options with you.
If you plan to have surgery, including dental surgery that needs a general anaesthetic; tell your doctor or dentist that you are taking CANDESAN COMBI.
Tell your doctor if you plan to have an examination such as an X-ray or a scan requiring an injection of iodinated contrast (dye) that you are taking CANDESAN COMBI.
If you have had skin cancer or if you develop a suspicious skin lesion during treatment with ATACAND PLUS, tell your doctor or pharmacist. Treatment with hydrochlorothiazide, particularly long-term use with high doses, may increase the risk of some types of skin and lip cancer (nonmelanoma skin cancer). Limit exposure to sunlight and protect your skin when exposed to sun while taking CANDESAN COMBI.
If you develop any severe shortness of breath or difficulty breathing after taking medicine, seek medical attention immediately.
Be sure to keep all of your doctor's appointments so that your progress can be checked. Your doctor will check your progress and may want to take some tests (e.g. blood tests, blood pressure) from time to time. These tests may help to prevent side effects.
Things you must not do
Do not use CANDESAN COMBI to treat any other conditions unless your doctor tells you to.
Do not give CANDESAN COMBI to anyone else, even if they have symptoms that seem similar to yours.
Do not stop taking CANDESAN COMBI unless you have discussed it with your doctor.
Things to be careful of
Move slowly when getting out of bed or standing up if you feel faint, dizzy or light-headed.
Be careful driving or operating machinery until you know how CANDESAN COMBI affects you.
You may feel dizzy when you start taking CANDESAN COMBI due to the drop in your blood pressure.
Drink plenty of water while you are using CANDESAN COMBI, especially if you sweat a lot.
Please talk to your doctor or pharmacist about these possibilities if you think they may bother you.
Side effects
Tell your doctor or pharmacist as soon as possible if you do not feel well while you are taking CANDESAN COMBI.
CANDESAN COMBI helps most people with high blood pressure, but it may have unwanted side effects in a few people.
All medicines can have side effects. Sometimes they are serious, most of the time they are not. You may need medical treatment if you get some of the side effects.
Ask your doctor or pharmacist to answer any questions you may have.
Tell your doctor if you notice any of the following and they worry you:
- headache or dizziness
- chest, throat or sinus infection
- flu-like symptoms or infections
- feeling sick (nausea) or vomiting
- back pain
- urinary tract infection
- feeling tired
- stomach ache
- symptoms of sunburn which happens more quickly than normal.
These side effects are usually mild.
Tell your doctor as soon as possible if you notice any of the following:
- rapid heartbeats
- aching muscles, tenderness or weakness in the muscles
- suspicious skin lesions
The above list includes serious side effects that may require medical attention. Serious side effects are rare.
If any of the following happen, tell your doctor immediately or go to Accident and Emergency at your nearest hospital:
- swelling of the face, lips, tongue or throat
- swelling of hands, feet or ankles
- harsh sounds when breathing
- rash, itching or hives
- easy bruising or bleeding more easily than normal
- feel extremely tired
- yellowing of the skin and/or eyes
- signs of frequent infections such as fever, severe chills, sore throat or mouth ulcers
- worsening of kidney function (including passing little or no urine, drowsiness, nausea, vomiting, breathlessness, loss of appetite and weakness (especially in patients with existing kidney problems or heart failure)
- changes in your potassium, sodium and red or white blood cell levels may occur. Such changes are usually detected by a blood test
- decrease in vision or pain in your eyes due to high pressure [possible signs of fluid accumulation in the vascular layer of the eye (choroidal effusion) or acute angle-closure glaucoma]
- symptoms that may indicate high potassium levels in the blood include nausea, diarrhoea, muscle weakness and changes in heart rhythm.
- Acute respiratory distress (very rare): signs include severe shortness of breath, fever, weakness and confusion.
These are very rare but serious side effects. If you have them, you may have had a serious reaction to the medicine. You may need urgent medical attention or hospitalisation.
Tell your doctor if you notice anything else that is making you feel unwell. Some people may get other side effects while taking CANDESAN COMBI.
After using CANDESAN COMBI
Storage
Keep your tablets in the blister pack until it is time to take them. If you take CANDESAN COMBI out of the blister pack it will not keep well.
Keep CANDESAN COMBI where children cannot reach it. A locked cupboard at least one-and-a-half metres above the ground is a good place to store medicines.
Keep your tablets in a cool dry place where the temperature stays below 25°C.
Do not store CANDESAN COMBI or any other medicine in the bathroom or near a sink.
Do not leave CANDESAN COMBI in the car or on window sills. Heat and dampness can destroy some medicines.
Disposal
If your doctor tells you to stop taking CANDESAN COMBI, or your tablets have passed their expiry date, ask your pharmacist what to do with any that are left over.
Product description
What it looks like
CANDESAN COMBI comes in 3 strengths of tablets:
- CANDESAN COMBI 16/12.5 – light pink, oval, biconvex tablet with ‘L3’ & ‘02’ on either side of break line on one side and a break line on the other side
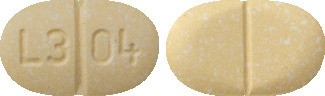
- CANDESAN COMBI 32/12.5 – light yellow, oval, biconvex tablet with ‘L3’ & ‘04’ on either side of break line on one side and a break line on the other side
- CANDESAN COMBI 32/25 – light pink, oval, biconvex tablet with ‘L3’ & ‘04’ on either side of break line on one side and a break line on the other side
Each Aluminium/Aluminium foil blister pack contains 30 tablets.
Ingredients
The active ingredients in CANDESAN COMBI are candesartan cilexetil and hydrochlorothiazide.
- each CANDESAN COMBI 16/12.5 tablet contains 16 mg of candesartan cilexetil and 12.5 mg of hydrochlorothiazide
- each CANDESAN COMBI 32/12.5 tablet contains 32 mg of candesartan cilexetil and 12.5 mg of hydrochlorothiazide
- each CANDESAN COMBI 32/25 tablet contains 32 mg of candesartan cilexetil and 25 mg of hydrochlorothiazide.
The tablets also contain:
- lactose monohydrate
- carmellose calcium
- maize starch
- macrogol 8000
- hyprolose
- magnesium stearate
- Pigment Blend PB-24880 Pink (16/12.5 mg and 32/25 tablet only)
- yellow colouring (iron oxide yellow and lactose monohydrate) (32/12.5 mg tablet only).
The tablets do not contain gluten, sucrose, tartrazine or any other azo dyes. Contains sugars as lactose.
Sponsor
Arrotex Pharmaceuticals Pty Ltd
15-17 Chapel Street
Cremorne, VIC 3121
Australia
www.arrotex.com.au
Australian registration numbers:
CANDESAN COMBI 16/12.5 – AUST R 204577
CANDESAN COMBI 32/12.5 – AUST R 204578
CANDESAN COMBI 32/25 – AUST R 204579
Date of Revision:
July 2023
Published by MIMS September 2023
 The following clinical adverse events occurred with a frequency of 0.5% to < 1% with no occurrence in the placebo group: AV-block, vomiting.
The following clinical adverse events occurred with a frequency of 0.5% to < 1% with no occurrence in the placebo group: AV-block, vomiting.
 The molecular weight is 610.67.
The molecular weight is 610.67. The molecular weight is 297.7.
The molecular weight is 297.7.